
Making Cocaine Rehab Work: A Guide for Busy Adults

Key Takeaways
- Structured outpatient care through PHP, IOP, or standard outpatient can match inpatient effectiveness for most adults while preserving work, family, and routine 5.
- No FDA-approved medication exists for cocaine use disorder, so behavioral therapy—especially contingency management, CBT, and motivational interviewing—does the real clinical work 1, 12.
- Plan for roughly 90 days of active treatment, since that's the minimum window where new routines and relapse-prevention skills become durable 14, 15.
- Care coordination across your PCP, prescriber, therapist, and EAP—plus federal confidentiality protections—lets treatment fit around a job and family without forced disclosure 7.
What Real Treatment Looks Like When You Can't Disappear for 30 Days
You probably found this page late at night, after a bad week, wondering if getting help means losing your job, your custody schedule, or the small thread of normal you've been holding onto. That fear is real. So is this: you don't have to vanish into a 30-day facility to get serious cocaine treatment that actually works.
For most adults with cocaine use disorder, the strongest evidence points to structured outpatient care delivered in partial hospitalization (PHP), intensive outpatient (IOP), or standard outpatient (OP) programs. These aren't watered-down options. An evidence review of intensive outpatient programs found they are as effective as inpatient treatment for most people, while letting you sleep in your own bed and keep showing up for work and family 5. The clinical engine inside those programs is behavioral therapy, because no medication has been FDA-approved for cocaine use disorder 1, 10. That fact changes the whole picture: the work happens in therapy rooms and group sessions, not in a prescription.
Here's what to expect in this guide. You'll see which therapies move the needle, how PHP, IOP, and OP differ in hours and duration, where medications might still fit as add-ons, and a realistic 90-day picture. The goal is simple: treat this as a scheduling and care-coordination puzzle with known answers, not a referendum on your willpower.
The Therapies That Actually Move the Needle
Why Behavioral Therapy Carries the Weight (And No Pill Replaces It)
Here's the part that surprises most people: there is no FDA-approved medication for cocaine use disorder. None. For opioids and alcohol, doctors have prescription tools that quiet cravings at a biological level. For cocaine, the science isn't there yet 1, 10. That's not a reason to lose hope. It's a reason to understand where the real work happens.
The work happens in therapy. Psychosocial treatment is the current standard of care for cocaine use disorder, and the evidence behind it is strong 1. A 2024 systematic review of psychosocial interventions for stimulant use disorder found high-certainty evidence that these therapies reduce dropout and cut stimulant use compared with no treatment at all 2. Translation: people who engage with structured behavioral care stay in treatment longer and use less. That matters more than any single technique.
What does this look like day-to-day? A combination of group therapy, individual counseling, and sometimes family sessions, usually delivered through intensive outpatient programming that runs several days a week 1. You learn to spot the cue that makes you reach for the phone. You practice what to say when a friend offers. You build a new map for your week. The therapy room is where cocaine recovery is actually built — not in a pharmacy, and not on willpower alone.
Contingency Management: The Current Standard of Care
If you've never heard of contingency management, you're not alone. Most consumer-facing rehab websites skip it entirely. But the 2024 ASAM/AAAP Clinical Practice Guideline names contingency management as the current standard of care for stimulant use disorder, including cocaine 12, 13. That's the highest-quality consensus we have, and it deserves a clear explanation.
Contingency management is simple in theory. You provide a clean urine sample. You earn a tangible reward — often a voucher, a small gift card, or a prize draw. Over weeks, the rewards grow if you keep submitting negative tests. The structure rewires the short-term math your brain runs every day. Cocaine hijacks your reward system; contingency management gives that system something else to chase.
It sounds almost too simple to work. It works anyway. Researchers have studied it for decades across multiple settings, and it consistently shows up in evidence syntheses as one of the most reliable tools for stimulant use disorder 3, 10.
A few honest notes. Rewards are modest, not life-changing. The structure requires showing up for testing, which is part of why programs build it into the weekly schedule. And like any therapy, contingency management works best when paired with the rest of your treatment plan — counseling, group, and the slower behavior change that comes with it.
CBT and Motivational Interviewing in Practice
Cognitive behavioral therapy, or CBT, is the workhorse of cocaine treatment. In a session, your therapist helps you map the chain that leads from a normal Tuesday to a craving you can't shake. The argument with your partner. The drive home past a familiar exit. The numb feeling that hits when you sit down on the couch. Once you can see the chain, you can interrupt it — earlier, on purpose, with a plan you wrote down when you weren't in crisis.
CBT also gives you a vocabulary for the lies cocaine tells you. "Just one line will help me get through this deadline." "I can handle it this weekend." "I'll stop after the holidays." You learn to catch the thought, name it, and answer it. That sounds small. It isn't. It's the difference between a hard Tuesday night and a relapse.
Motivational interviewing is the conversation underneath all of this. NIDA's research guide notes that motivational enhancement therapy helps people resolve the ambivalence that almost everyone brings into treatment 15. You can want to quit and want to use at the same time. A good therapist doesn't argue with the part of you that's still attached to cocaine. They ask questions that let your own reasons for changing come forward. That's where lasting motivation comes from — not from a lecture, but from your own voice.
What Trauma-Informed Care Feels Like in a Session
Trauma-informed care is a phrase that gets tossed around. Here's what it actually looks like in a room.
You walk in. The chairs aren't arranged so you're facing a wall. Your therapist asks where you'd like to sit. They tell you what's going to happen in the session before it happens, so nothing comes out of nowhere. If you don't want to talk about something today, that's a complete sentence. You won't be pushed to relive the worst day of your life on a clinician's timeline.
When you describe a cocaine binge, no one flinches. No one calls you weak. The questions stay curious — what did the drug do for you, what were you trying to quiet, what happened in your life before the use started? Trauma-informed care assumes that substance use is often an answer your nervous system found to a problem nobody helped you solve.
For adults who've been judged in past treatment settings, this matters more than any specific therapy technique. You can't do hard behavioral work if you don't feel safe enough to tell the truth. Safety in the room is the floor everything else gets built on.
Choosing the Right Level of Care for Your Week
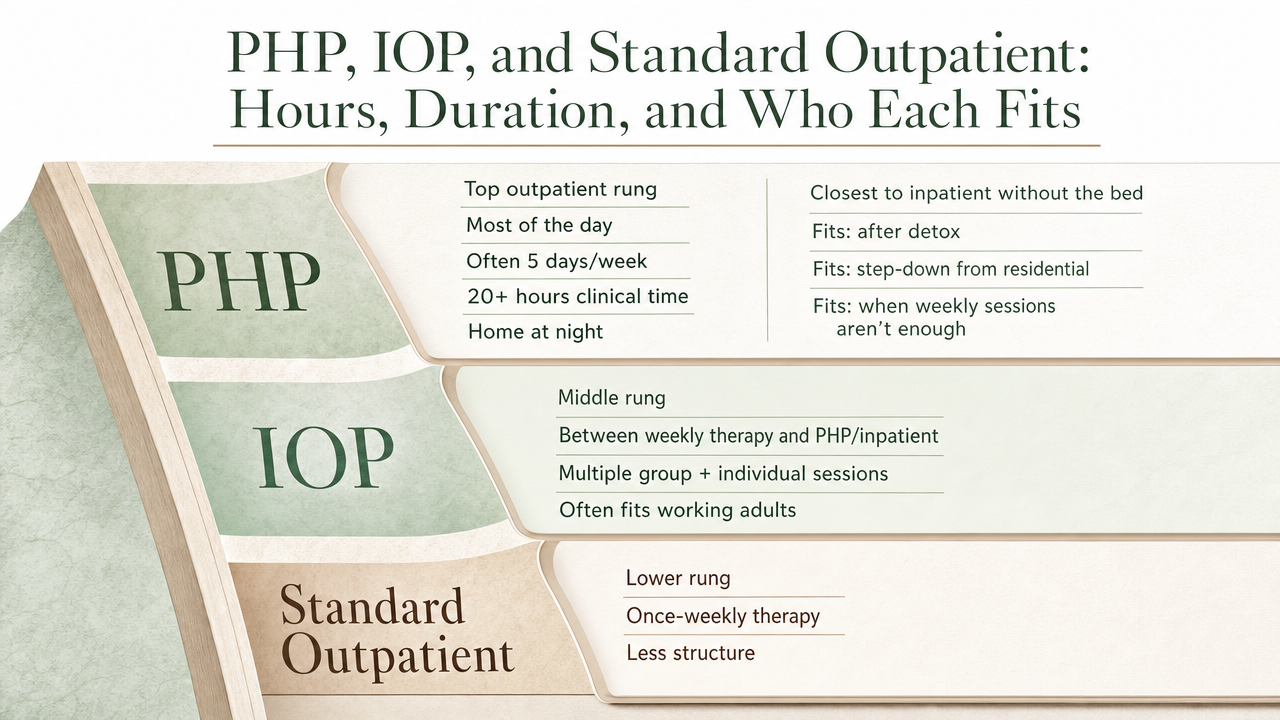
PHP, IOP, and Standard Outpatient: Hours, Duration, and Who Each Fits
Outpatient care isn't one thing. It's a ladder, and the rung you start on depends on how much structure your week needs to hold steady.
Partial hospitalization (PHP) sits at the top of the outpatient ladder. You spend most of the day at the program — often five days a week, roughly 20 or more hours of clinical time — and go home at night. It's the closest thing to inpatient without the bed. PHP fits if you're coming out of detox, stepping down from a residential stay, or your use has reached a point where a few weekly sessions won't catch you fast enough.
Intensive outpatient (IOP) is the middle rung and the one most working adults land on. Medicare describes IOP as a level of care that sits between once-weekly therapy and inpatient or partial hospitalization, typically including multiple group and individual sessions and possible medication management 6. In practice, that usually means around 9 to 12 hours per week across three or four days. The IOT phase is commonly built around a 90-day minimum, because that's the length the evidence points to for meaningful behavior change 14, 15. Critically, an evidence review found IOPs can be as effective as inpatient treatment for most people while you live at home 5.
Standard outpatient (OP) is the bottom rung — usually one to two sessions a week. It's where many people land after IOP, or where you start if your use is less severe and your support at home is strong.
Fitting an IOP Schedule Around Work, Commute, and Pickup
Let's get specific, because this is the part that decides whether you actually start.
A common IOP track runs three evenings a week, three hours each — say Monday, Wednesday, and Thursday from 5:30 to 8:30 p.m. That's nine clinical hours, which lines up with how Medicare frames IOP as a level of care built on multiple weekly sessions of group and individual therapy 6. You leave work at five, grab something to eat in the car, sit in group from 5:30 to 8:30, and you're home by nine. Your boss doesn't need to know your evening plans. Your kids see you at breakfast and bedtime on most days.
Morning tracks work the same way in reverse — group from 7:00 to 10:00 a.m., then into the office by 10:30. Some programs run afternoon tracks for shift workers or parents whose mornings belong to school drop-off.
The 90-day frame matters here too 14. Three months of three evenings a week sounds like a lot until you compare it to the alternative: 30 days away from your job, your home, and the people who depend on you. An IOP schedule asks you to give up roughly nine hours a week of what was probably already chaotic time. The trade is real, and for most working adults it's the trade that lets treatment happen at all.
Where Medications Fit (And Where They Don't)
That said, a prescriber may still consider an off-label medication as an add-on to behavioral therapy. Topiramate is the one that shows up most often in the research. A 2025 systematic review and meta-analysis of randomized controlled trials found that topiramate produced a risk ratio of 2.83 (95% CI 1.68–4.76) for early cocaine abstinence compared with control, with similar retention and adverse event rates 4. In plain terms: in those trials, people taking topiramate were meaningfully more likely to hit early abstinence milestones than people on placebo. The same review also noted little impact on craving and unclear long-term benefit, so this is an early-window adjunct, not a cure 4.
If you also have a co-occurring condition — depression, anxiety, ADHD, or a sleep problem — medication for that condition can be a real part of your plan. Treating what's underneath the cocaine use often makes the behavioral work stick. The pattern that holds up across the evidence is consistent: therapy is the engine, and medication, when it fits, is the passenger.
The Hidden Lever: Care Coordination With Your Existing Providers
Most rehab pages skip this part, and it's the part that quietly decides whether your recovery sticks. Your treatment program doesn't exist on an island. You probably already have a primary care doctor, maybe a therapist you've seen on and off, possibly a prescriber managing anxiety meds or blood pressure. Your employer might have an EAP you've never used. Somewhere in there is a family member who keeps asking how you are. Coordinating across those people is the lever almost nobody talks about.
The Institute of Medicine put this plainly: treatment providers should build clinically effective linkages between mental health, substance use, and general medical care so information actually moves between them 7. In practice, that means your outpatient program asks for a release of information, then talks to your primary care doctor about what's happening, sends updates to your prescriber if you're on medication for depression or ADHD, and loops in your EAP if you're using one to protect your job. You sign what gets shared and with whom. Nothing moves without your say-so.
Why does this matter for cocaine recovery specifically? Because the things that pulled you toward cocaine rarely sit in one provider's chart. A sleep problem your PCP has been treating. Anxiety your therapist has been working on. Pain medication someone else is managing. When those providers don't talk, you become the messenger — and the messenger is the person who's exhausted and hiding things. Good care coordination takes that job off your plate.
It also makes the practical stuff easier. Your program can write a letter your HR department needs. Your prescriber knows what your treatment team is seeing each week. Your primary care doctor stops prescribing something that's working against your recovery. Recovery planning and care coordination, done well, is less a service line and more the connective tissue that keeps the rest of your life from working against the progress you're making in group on Tuesday night.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
A Realistic 90-Day Picture: What the First Three Months Look Like
Ninety days is the number that keeps showing up in the research, and it's worth understanding why. NIDA's principles guide notes that many people need at least three months in treatment to see meaningful change, and the IOT chapter in the NCBI continuum-of-care reference cites 90 days as the commonly recommended minimum for intensive outpatient work 14, 15. That's not arbitrary. It's roughly how long it takes for new routines to stop feeling like effort and start feeling like Tuesday.
The first 30 days are the hardest, and you should know that going in. Cocaine cravings hit harder when the structure is new, sleep is uneven, and you're still untangling the social patterns around your use. In a typical IOP track, you're in group three evenings a week, meeting your individual counselor weekly, and probably doing urine testing tied to contingency management. You'll feel exposed. You'll want to skip a session. Showing up anyway is the work in month one.
Days 31 to 60 tend to feel different. The group starts to feel like people, not strangers. You catch a craving earlier than you used to. You have a plan for Friday night that isn't just white-knuckling. Your therapist starts pushing on the stuff underneath — the anxiety, the grief, the relationship that's been quietly falling apart. This is where dual diagnosis work often deepens, and where care coordination with your prescriber or primary care doctor starts paying off 7.
Days 61 to 90 are about transition. You may step down from IOP to standard outpatient — one or two sessions a week — while keeping the relapse-prevention plan you built. Some people stay longer in IOP; some move into alumni support or a sober-living arrangement. The point isn't to graduate on day 90. The point is that by then, you've built enough of a structure that recovery is something you live inside, not something you're constantly fighting for.
Protecting Your Job, Your Privacy, and Your Family During Treatment
The thing keeping most adults out of treatment isn't the treatment itself. It's the fear of what happens around it. Will HR find out? Will your ex use this in court? Will your mother-in-law have something to say at Thanksgiving? Those fears are reasonable, and the answers are mostly better than you think.
On the job front, your records are protected. Outpatient programs operate under federal confidentiality rules that are stricter than standard medical privacy. Nothing goes to your employer without a release you sign, and even then, you control what gets shared and what stays out. If you're using an EAP, the program can coordinate with the EAP counselor without disclosing clinical details to your employer 7. If you need documentation for FMLA or short-term leave, a clinician can write what's needed without naming cocaine specifically on most forms. Evening and morning IOP tracks exist precisely so you don't have to explain a three-hour gap in your workday.
For family, the conversation is harder than the paperwork. You don't owe everyone the full story. You do owe the people who live with you enough information to be on your side — when you'll be gone, what to expect on hard nights, and what helps. A good program offers family sessions when you want them and stays out of the way when you don't.
How to Start This Week Without Blowing Up Your Schedule
Starting treatment doesn't require a grand announcement. It requires one phone call and a calendar.
Here's a workable plan for the next seven days. Today or tomorrow, call an outpatient program directly and ask for an assessment. If you don't know where to begin, SAMHSA's free, confidential helpline runs 24/7 and can point you toward local options 8. An assessment is usually 60 to 90 minutes — in person or over video — and it's the conversation that determines whether PHP, IOP, or standard outpatient fits your situation. Bring a rough sense of how often you've been using, what you've already tried, and any medications you take.
While you're waiting on the assessment, do two small things. Look at your calendar and find the three-hour blocks you could protect — early morning, evening, or a mix. Check your insurance card and call the number on the back to ask what's covered for outpatient substance use treatment.
If you're in southern Maine, Coastal Recovery Partners in South Portland offers PHP, IOP, and standard outpatient tracks with morning, afternoon, and evening options built for adults who can't step away from work. One call starts the clock. You don't have to have it figured out before you pick up the phone.
Frequently Asked Questions
Can I get real cocaine rehab without taking 30 days off work?
Yes. Intensive outpatient and partial hospitalization programs let you live at home and keep working while getting clinically serious treatment. An evidence review found IOPs can be as effective as inpatient care for most people 5. Evening and morning tracks are built so you don't have to disclose treatment to your employer to attend.
Is there an FDA-approved medication for cocaine use disorder?
No. Unlike opioid or alcohol use disorder, no medication has been FDA-approved for cocaine use disorder, which is why psychosocial treatment is the standard of care 1, 10. A prescriber may consider off-label options as add-ons to therapy, but any clinic promising a pill that fixes cocaine cravings is overstating what the science currently supports.
How long does outpatient cocaine treatment actually take?
The commonly recommended minimum for intensive outpatient work is around 90 days, and NIDA notes many people need at least three months in treatment to see meaningful change 14, 15. After IOP, many people step down to standard outpatient — one or two sessions a week — and continue for several more months. Recovery doesn't end on day 90; the active structure shifts.
What's the difference between PHP, IOP, and standard outpatient care?
PHP is the most intensive outpatient level — most of the day, several days a week. IOP sits in the middle, typically around 9 to 12 hours weekly across three or four days, with group and individual therapy and possible medication management 6. Standard outpatient is one or two sessions a week. The right starting point depends on how much structure your week needs to stay safe.
Will my employer or family find out I'm in treatment?
Not unless you decide they should. Substance use treatment records carry stricter federal confidentiality protections than general medical records. Nothing leaves your program without a release you sign, and you control what gets shared and with whom 7. If you use an EAP or need FMLA paperwork, a clinician can coordinate that without naming cocaine on most forms.
How do I start treatment this week if I'm not sure where to begin?
Call an outpatient program directly and ask for an assessment, usually a 60 to 90 minute conversation that determines the right level of care. If you don't know where to start, SAMHSA's free, confidential helpline runs 24/7 and provides referrals to local treatment options 8. While you wait, check your insurance and protect a few three-hour blocks on your calendar.
References
- The treatment of cocaine use disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC6795516/
- Psychosocial interventions for stimulant use disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC10867898/
- Navigating Evidence, Challenges, and Caution in the Treatment of Stimulant Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC10605120/
- Topiramate Therapy in Cocaine Use Disorder: A Systematic Review and Meta-analysis of Randomized Controlled Trials. https://pubmed.ncbi.nlm.nih.gov/41047145/
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Intensive Outpatient Program Services. https://www.medicare.gov/coverage/mental-health-care-outpatient-intensive-outpatient-program-services
- Coordinating Care for Better Mental, Substance-Use, and General Health. https://www.ncbi.nlm.nih.gov/books/NBK19833/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Treatment of Stimulant Use Disorders - SAMHSA. https://www.samhsa.gov/resource/ebp/treatment-stimulant-use-disorders
- Treatment and Recovery | National Institute on Drug Abuse (NIDA). https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
- Treatment of Substance Use Disorders | Overdose Prevention - CDC. https://www.cdc.gov/overdose-prevention/treatment/index.html
- The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. https://pubmed.ncbi.nlm.nih.gov/38669101/
- The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. http://stacks.cdc.gov/view/cdc/156927
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Principles of Drug Addiction: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- Treatment for Stimulant Use Disorders - NCBI Bookshelf - NIH. https://www.ncbi.nlm.nih.gov/books/NBK576541/



