
How Long Is PHP Treatment?

Key Takeaways
- Most adults complete PHP in roughly 2 to 6 weeks, attending about 5 days a week for 4 to 6 hours daily, though the exact length isn't fixed.
- PHP is defined by intensity, not duration—at least 20 hours of clinical contact weekly—because it serves people who would otherwise need inpatient care 6.
- Length of stay shifts with three factors: clinical progress and stabilization, co-occurring conditions, and rolling insurance reviews that authorize care in 5-to-7-day cycles based on medical necessity 9.
- PHP is one step in a stepped continuum—most adults transition to IOP at roughly 9 to 12 hours a week, then standard outpatient and aftercare 8.
The Honest Answer: Weeks, Not a Fixed Calendar
If you're looking for a clean number, here it is: most adults complete a Partial Hospitalization Program in roughly 2 to 6 weeks, attending treatment about 5 days a week for 4 to 6 hours a day. That's the realistic range you can plan around for time off, childcare swaps, and the conversation you're dreading with your manager.
But PHP isn't sold in a fixed package of days, and anyone who tells you otherwise is simplifying for a brochure. Federal payers and clinical bodies define PHP by intensity, not by length of stay. Medicare, for instance, doesn't cover a preset number of days at all. Coverage depends on whether you'd otherwise need inpatient care and whether you're still making clinical progress at that level 9. The consensus clinical definition treats PHP as a structured outpatient program for active treatment of a serious condition—short-term by design, not residential, not casual 10.
So your real length of stay gets decided by three things working together: how you're actually doing week to week, what your insurance authorizes after each utilization review, and what your clinical team sees in the room. Some people stabilize in 10 to 15 treatment days. Others need a longer runway because of withdrawal, a co-occurring mental health condition, or a home situation that isn't safe yet.
Yes, that ambiguity is uncomfortable when you're trying to block a calendar. The rest of this guide gives you the actual variables that move the number—so you can plan with your eyes open, not guess.
What a PHP Week Actually Looks Like
Weekly Hours, Daily Schedule, and Why 20 Is the Floor
When you hear “partial hospitalization,” picture a full workweek of treatment that happens during business hours and lets you sleep at home. That's the shape of it. The intensity is real, but it's bounded.
The 20-hour-per-week figure isn't a guess or a marketing average—it's the floor written into how these programs are defined. ASAM Level 2.5 partial hospitalization, as codified in state Medicaid rules, requires a minimum of 20 hours per week of skilled treatment and at least 5 service hours per service day, delivered across at least 5 days per week 6. Pennsylvania's ASAM guidance echoes the same baseline: 20 or more hours of clinically intensive programming each week, sometimes called “day treatment” 7. If a program calls itself PHP but only schedules you for 12 hours a week, it isn't actually PHP—it's intensive outpatient wearing the wrong name tag.
What does that look like on a calendar? In most adult programs, you'll arrive in the morning—often around 9:00 a.m.—and leave by mid-afternoon, with a lunch break built in. Some programs run an afternoon or early-evening track to make room for people with caregiving responsibilities or specific work arrangements, though daytime is the standard. You're typically on-site (or on a video platform, for virtual PHP) Monday through Friday.
Here's why 20 is the floor and not the ceiling: PHPs are designed for people who would otherwise need inpatient care. That's the threshold federal payers use 9. To safely keep you out of a hospital bed, the program has to provide enough structured contact each week to actually move symptoms in the right direction. Anything less and the level of care isn't doing its job.
One practical note for planning: those 20+ hours are clinical contact hours. They don't include your commute, the time you spend decompressing after a hard group, or any homework your therapist assigns between sessions. When you're blocking your calendar, give yourself an honest buffer—most people find the real time cost is closer to 30 hours a week once travel and recovery are factored in. That's not a reason to talk yourself out of it. It's a reason to plan for it with both eyes open.
A Sample Day Inside a PHP
Abstract hours are hard to plan around. A sample day is easier. Programs vary, but a typical Tuesday in an adult PHP looks something like this:
- 9:00–10:15 a.m. — Morning check-in and process group.
- You sit with the same small group of peers most days. The clinician leads a structured check-in: how you slept, cravings or mood shifts since yesterday, what's on deck this week. This is where patterns get noticed before they snowball.
- 10:30–11:45 a.m. — Skills group.
- This is the teaching block. Cognitive behavioral therapy (CBT) tools for catching the thoughts that pull you toward use. Dialectical behavior therapy (DBT) skills for riding out intense emotions without acting on them. Relapse prevention planning. You'll leave with something you can actually use that night.
- 11:45 a.m.–12:30 p.m. — Lunch.
- Built into the schedule. Some programs eat together; others give you space to step away.
- 12:30–1:30 p.m. — Individual therapy or psychiatry (one to two times a week).
- On days without individual sessions, this slot is often used for case management, medication-assisted treatment check-ins, or a focused topic group.
- 1:45–3:00 p.m. — Afternoon group.
- This shifts day to day—trauma-informed psychoeducation, communication and family work, mindfulness or grounding practice, life-skills planning. By Friday, the week's themes start to connect.
Add it up and you're at roughly 5 clinical hours, five days a week. That's where the 20-plus-hour number comes from in real life. It's intense, and it's meant to be. PHP exists for the stretch when you need active treatment of a serious condition in a structured outpatient setting 10—not maintenance, not a check-in once a week. The good news is that this intensity is also what makes the program short.
What Actually Moves Your Length of Stay Up or Down
Clinical Variables: Progress, Stabilization, and Co-Occurring Conditions
Your clinical team isn't sitting on a stopwatch. They're watching specific things, and those things decide how long you stay.
The first one is stabilization. If you came into PHP fresh off withdrawal, with sleep wrecked, cravings spiking, and a mood that's all over the map, the first 7 to 10 days are mostly about getting your body and brain back to a baseline where therapy can actually land. You can't do trauma work on no sleep. You can't apply CBT skills when you're white-knuckling the hour. Once that baseline holds—steady sleep, fewer cravings, more emotional bandwidth—treatment shifts into the real work, and the clock starts moving differently.
The second is co-occurring conditions. If you're dealing with substance use plus a mental health diagnosis like depression, anxiety, PTSD, or bipolar disorder, your stay is usually longer than someone working on a single issue. That's not a punishment. It's math. Two things take more time to treat than one, and they often feed each other in ways that need separate attention. PHP is built to handle this kind of integrated care, which is part of why it's used as an alternative to inpatient stabilization in the first place 2.
The third is progress itself. Your treatment team measures it weekly: Are you using the skills outside of group? Sleeping? Showing up on time? Being honest in individual sessions? Tolerating uncomfortable feelings without using? When those answers start trending in the right direction consistently, you're getting close to step-down. When they're not, the team adjusts—sometimes that means more time at this level, sometimes it means changing what's happening in the room.
Payer Variables: Medical Necessity and Authorization Cycles
Insurance shapes your timeline in a way that's worth understanding upfront, because it's where a lot of the surprise comes from.
Here's the core rule: most major payers, Medicare included, don't cover a fixed number of PHP days. Coverage hinges on medical necessity—the idea that without this level of care, you'd otherwise need inpatient treatment 9. As long as that's true and you're making progress, your stay continues. When it's no longer true, coverage steps down with you.
How does the insurance company actually know? Through utilization review. Your treatment team submits documentation—usually after an initial authorization of a set number of days, then in rolling cycles of about 5 to 7 days at a time. A reviewer on the payer side looks at your symptoms, your progress, your safety, and your treatment plan, then approves another stretch or asks for a step-down. This is normal. It's not a sign anything is wrong. It's the rhythm PHP runs on.
What this means for you: your length of stay can shift mid-program. You might come in expecting four weeks and find your team and your insurer agreeing you're ready to step down to IOP at week three. Or you might need an extra week your initial estimate didn't include. CMS's own analysis of PHP utilization patterns has shown wide variability in episode length, shaped heavily by how payer rules and local practice intersect 3.
The practical move is to ask two questions before you start: how often does this program submit for re-authorization, and what happens if my insurer denies an extension? Good programs have answers ready, including a clear plan to advocate clinically for more time when it's warranted and a smooth handoff into IOP if it's not. You shouldn't have to figure out the appeals process while you're in the middle of recovery.
The Outlier: When PHP-Style Care Runs Months, Not Weeks
If you've searched around online, you've probably seen length-of-stay numbers that don't agree with each other. One page says two weeks. Another says nine months. Both can be technically accurate, and the gap deserves a real explanation.
A 2025 Ohio state report on partial hospitalization documented two PHP-related programs where the average length of stay was nine months 4. That's not a typo, and it's not typical adult substance use PHP. Those programs reflect a long-term rehabilitative model—closer to a structured day-rehab setting for people with chronic, complex needs who require extended therapeutic structure outside of an inpatient bed. They're called partial hospitalization because of how they're licensed and reimbursed, but their treatment philosophy is fundamentally different from the 2-to-6-week stabilization model most working adults are looking at.
Most adult PHPs for substance use sit firmly in the weeks-not-months range. The Ohio outlier is useful precisely because it shows the full spread: PHP as a regulatory category is wide, and what matters for your planning is the specific program you're talking to.
When you call a program, ask directly: “What's your typical length of stay for someone with my situation?” A straight answer—a range, not a sales pitch—tells you a lot about whether you're looking at short-term stabilization with a step-down plan or a longer rehabilitative track. Both can be the right answer for the right person. They're just not the same thing, and you deserve to know which one you're signing up for before you start rearranging your life around it.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Planning PHP Around Work and Family Logistics
Time-Off Math: Mornings, Afternoons, and the Realistic Work Question
Let's do the math you're actually trying to do. If your program runs roughly four weeks at 5 days a week, that's about 20 weekdays of treatment. Add buffer for commute and decompression, and you're looking at most of a typical workday gone, Monday through Friday, for somewhere between two and six weeks depending on how things go.
For a lot of working adults, that doesn't fit around a full-time job. It replaces a full-time job for the duration. The good news is that the duration is finite by design—PHP is built as a short, intensive episode followed by lower-intensity care 1. You're not signing up for an indefinite leave.
Here are the routes people actually use, in plain terms:
- Short-term medical leave. Many employers offer some form of protected leave for a serious health condition. Substance use and co-occurring mental health diagnoses generally qualify. Your HR team or your treatment program's care coordinator can help you sort out paperwork without you having to disclose more than the law requires.
- Vacation, PTO, or unpaid leave stacked together. For a 2-to-3-week stay, some people piece together existing time off. It's not glamorous, but it works.
- Reduced or modified duties. A small number of adults work a few evening or weekend hours around PHP, especially in the last week or two when things have stabilized. Talk to your clinical team before adding any work hours. They'll tell you honestly when you have the bandwidth.
- Afternoon or evening tracks. Some programs run a non-standard schedule for people with daytime responsibilities. These exist, but they're less common, so ask early in the call.
One thing to skip worrying about: you don't owe your employer a clinical narrative. “I'm taking medical leave under my doctor's care” is a complete sentence. The hardest part of this conversation is usually the anticipation. The actual exchange tends to be shorter, and quieter, than the version that plays on loop at 2 a.m.
Virtual vs In-Person PHP: Does Format Change Your Time Commitment?
Format doesn't change the weekly hours—virtual PHP runs at the same intensity as in-person care, because the standard is defined by clinical contact time, not by where you sit during it. What changes is the friction around those hours.
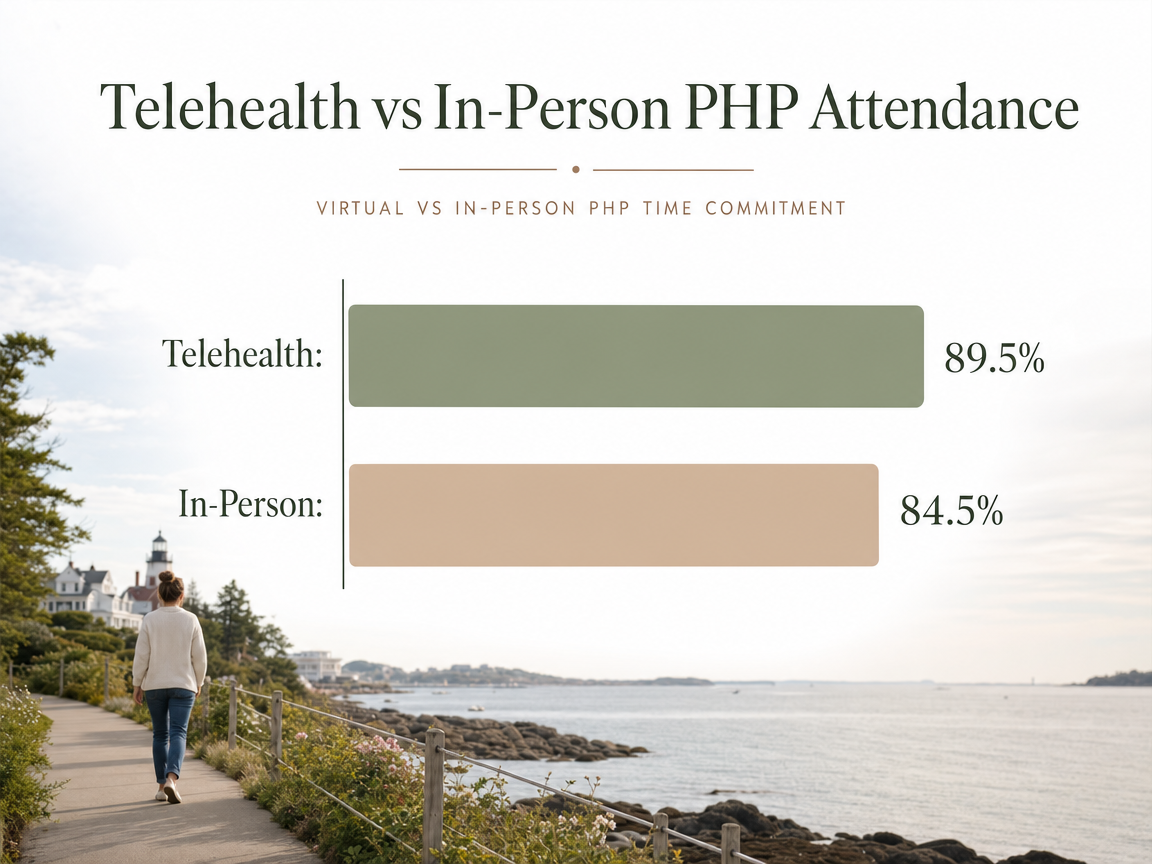
Virtual PHP cuts commuting, parking, and the awkward 20-minute gap between leaving home and starting group. For someone managing childcare pickups, a partner's work schedule, or a longer drive from a rural part of the region, that saved time is the difference between “possible” and “not possible.” A 2022 peer-reviewed study comparing a virtual adult PHP with the same program delivered in person found that attendance was higher in the telehealth format—89.5% versus 84.5%—along with lower hospitalization rates and similar symptom outcomes 5. A 5-point attendance gap is meaningful when you're stringing together four weeks of daily treatment. Missing two days a week versus missing one changes how the program lands.
That said, virtual isn't automatically better for everyone. If your home isn't private, if your housemates are using, or if you focus better when you've physically left the house, in-person care will likely serve you more. Some people start virtual and switch to in-person, or the reverse. The format question is worth asking on your first call.
On length of stay: there's no evidence that virtual PHP is shorter or longer than in-person. The same clinical and payer rules apply. What format buys you is a better shot at showing up for every day you're scheduled, which is what actually moves your treatment forward.
After PHP: The Step-Down Map Through IOP and Outpatient
Finishing PHP is a real milestone. It's also the start of the next phase, not the finish line. Treatment is built as a stepped continuum, and the whole design assumes you'll move down through lower-intensity levels as your stability grows 1.
Here's how that map usually looks for an adult coming out of PHP:
Intensive Outpatient Program (IOP). The most common next step. You drop from roughly 20+ hours a week to about 9 to 12 hours a week—typically three sessions a week, three hours each, often available in morning or evening tracks. IOP is where a lot of working adults transition back to a job, sometimes part-time at first. The clinical focus shifts from active stabilization to early recovery: practicing skills in real life, handling triggers at work and at home, deepening relapse prevention. IOP commonly runs 8 to 12 weeks, though, like PHP, the actual length is driven by progress rather than a fixed term 8.
Standard Outpatient (OP). After IOP, most people step down to weekly or twice-weekly individual therapy, group sessions, and ongoing medication management if you're using MAT. This is the maintenance and community-support phase—months of lighter-touch care that protects what you built in the more intensive levels 8.
Aftercare and alumni support. Recovery doesn't end when formal sessions stop. Many programs offer alumni groups, peer support, and check-ins that you can lean on for years if you want. There's no clock on that piece.
The honest framing: PHP gets you stable. IOP teaches you to carry it. Outpatient helps you keep it. You're not racing through the levels—you're letting each one do its job. A care coordinator can help you sequence the handoffs so there's no gap between PHP discharge and IOP start, which is the moment a lot of people quietly fall off. Coastal Recovery Partners structures its programs around exactly this kind of step-down, with MAT, dual diagnosis support, and trauma-informed care that travels with you across the levels rather than restarting at each one.
A Realistic Week-by-Week Picture for a Working Adult
Here's what the arc actually feels like, week by week, for an adult walking into PHP with a job, a family, and a life that didn't pause to make room for treatment.
Week 1 — Landing. The first few days are the hardest, and not because of the therapy. You're adjusting to a new schedule, meeting your group, and getting your body back to a baseline. Sleep is often still off. Cravings can spike in the evenings. Skills work has started, but it hasn't sunk in yet. Most people use this week to lock in childcare, finalize their leave paperwork, and let the people who need to know what's happening. You're showing up. That's the win.
Week 2 — Traction. Things start clicking. You know the rhythm of the day. The CBT and DBT skills you learned in week one show up uninvited in real moments—a tense text from a family member, a craving on the drive home—and you actually use them. Individual therapy goes deeper because there's enough stability to handle it. Your treatment team is watching for exactly this shift.
Weeks 3 to 4 — Building and deciding. The conversation about step-down starts here. Your team and your insurer are reviewing progress in rolling cycles, and a step to IOP is usually on the table by the end of week three or four if things are holding. Some people stay through week six. Some are ready earlier. Either is fine.
Weeks 5 onward — Transitioning back. Once you step down to IOP, you're typically attending three sessions a week and easing back into work, often part-time at first. The skills you built in PHP get road-tested against ordinary life—which is the whole point. You're not done. You're moving from active treatment into early recovery, and the schedule finally bends back toward something that looks like your old calendar.
Frequently Asked Questions
How many weeks does PHP usually last for an adult?
For most adults, PHP runs about 2 to 6 weeks. Some people stabilize in 10 to 15 treatment days; others stay longer when withdrawal, a co-occurring mental health diagnosis, or home instability needs more time. The number isn't fixed by a schedule—it's driven by your week-to-week progress and your payer's medical-necessity reviews 9.
Can I work a job while attending PHP?
Not a full-time job, in most cases. PHP runs about 5 days a week during business hours, so it tends to replace work for the duration rather than fit around it. A handful of people manage a few evening or weekend hours, especially toward the end. Short-term medical leave, PTO, or unpaid leave usually covers the gap. Talk with your clinical team before adding work hours.
What determines whether my PHP stay gets extended or shortened?
Three things, working together. Your clinical progress—sleep, cravings, skill use, honesty in sessions. Your safety and stability at home. And your insurer's rolling utilization reviews, which approve care in short cycles based on medical necessity 9. If you're stable and using skills, step-down comes sooner. If symptoms or safety still need active treatment, your team can advocate for more time at this level.
Does insurance cover a set number of PHP days?
Generally, no. Medicare and most major payers cover PHP based on medical necessity, not a preset number of days 9. Your program submits documentation in rolling cycles—often every 5 to 7 days—and coverage continues as long as you'd otherwise need inpatient care and you're making progress. CMS data shows episode length varies widely by program and payer rules 3. Ask about re-authorization and appeals upfront.
What happens after PHP ends?
Most adults step down into an Intensive Outpatient Program (IOP), dropping to roughly 9 to 12 hours a week across three sessions, often with morning or evening tracks that allow a return to work 8. After IOP, standard outpatient takes over—weekly therapy, medication management if you're using MAT, and alumni or peer support. The whole continuum is built as stepped care, designed to lower intensity as stability grows 1.
Is virtual PHP shorter or different in length than in-person?
No. Virtual PHP runs at the same weekly intensity as in-person care, and the same clinical and payer rules govern length of stay. What changes is friction—no commute, easier childcare coordination—which tends to improve attendance. One peer-reviewed comparison found telehealth PHP had 89.5% attendance versus 84.5% in-person, along with lower hospitalization rates and similar symptom outcomes 5. Format affects how you show up, not how long you stay.
References
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Providing Crisis-oriented and Recovery-based Treatment in Partial Hospitalization Programs. https://pmc.ncbi.nlm.nih.gov/articles/PMC2848466/
- A Study of Partial Hospitalization Programs. https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/reports/downloads/Leung_PHP_PPS_2010.pdf
- Partial Hospitalization Study Report. https://dbh.ohio.gov/wps/portal/gov/dbh/research-and-data/data-and-reports/documents/partial-hospitalization-study-report
- Positive Outcomes in a Virtual Partial Hospitalization Program. https://pmc.ncbi.nlm.nih.gov/articles/PMC9395212/
- 12VAC30-130-5100. Partial hospitalization services (ASAM Level 2.5).. https://law.lis.virginia.gov/admincode/title12/agency30/chapter130/section5100/
- LEVEL 2.5 PARTIAL HOSPITILIZATION SERVICES BY SERVICE CHARACTERISTICS. https://www.pa.gov/content/dam/copapwp-pagov/en/ddap/documents/documents/asam/level%202.5%20self%20assessment.pdf
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Mental health care (partial hospitalization). https://www.medicare.gov/coverage/mental-health-care-partial-hospitalization
- Definition of partial hospitalization. The National Association of Private Psychiatric Hospitals and the American Association for Partial Hospitalization. https://pubmed.ncbi.nlm.nih.gov/10106610/



