
Exploring Your MDMA Addiction Treatment Options

Key Takeaways
- No FDA-approved medication exists for MDMA use disorder, so effective care centers on behavioral therapies like CBT, DBT, and relapse prevention rather than a daily pill 4, 9.
- Matching the level of care matters more than defaulting to residential rehab; most people start with standard or intensive outpatient and keep their job, school, or family routine intact 1.
- Treating MDMA alone rarely holds because anxiety, depression, trauma, and polysubstance use usually sit underneath, and 21.3% of drug-related ED visits in 2024 involved more than one substance 3.
- MDMA-assisted therapy is being studied for PTSD, not as a treatment for MDMA addiction, and the FDA advisory committee voted against approval in 2024 7, 8.
The Truth About MDMA Treatment Most Articles Skip
Here is the thing most articles about MDMA addiction treatment skip in the first paragraph: there is no FDA-approved medication for MDMA use disorder. None. You cannot walk into a clinic and get a patch, a daily pill, or an injection that treats MDMA the way methadone treats opioid dependence. That changes what "treatment" actually means for you.
If you have been searching for a quick medical fix, that news might feel like a door closing. It is not. It just means the real work happens somewhere else. The treatment that helps people stop using MDMA is built around structured behavioral care, mental health support for what the drug is often masking, and a recovery plan that fits your actual life 1. NIDA notes that people who use MDMA can develop tolerance, withdrawal-like aftereffects, and continued use despite knowing it is causing harm 4. Those are real patterns. They also respond to real, non-pharmaceutical help.
This guide walks you through what that looks like in plain terms. You will see how outpatient care levels actually differ, why treating MDMA almost always means treating something underneath it, and where the much-talked-about MDMA-assisted therapy research fits in (spoiler: it is not a treatment for MDMA addiction). No sales ladder. No scare tactics. Just the honest map you came here for.
Why Stopping MDMA Is Harder Than People Expect
The Tuesday Crash and What's Actually Happening
You probably know the pattern even if you've never put words to it. Saturday feels like the best night of your life. Sunday is hazy but okay. Then Tuesday hits, and you feel hollowed out, anxious, foggy, weirdly sad about nothing in particular. Sleep is off. Focus is gone. You snap at someone you love and can't explain why.
That is not a personal failing. NIDA describes heavy users experiencing"confusion, depression, sleep abnormalities, and problems with attention and memory"in the days after use 5. MDMA floods your brain with serotonin during the high, and your system needs days, sometimes longer, to rebuild that supply. The crash you feel midweek is partly the bill coming due.
Here is why that matters for stopping: the easiest way to feel better on a Tuesday is to use again on Friday. The drug solves the problem the drug created. NIDA notes that some people develop tolerance and continue using despite knowing it is causing harm 4. That loop is not weakness. It is chemistry meeting habit, and it is exactly what behavioral treatment is built to interrupt.
Signs Your Use Has Crossed a Line
There is no clean line between "recreational" and "a problem." It usually creeps. But a few patterns tend to show up before people are ready to name them out loud.
- You need more to feel the same thing.
- You promised yourself you'd only use at certain events, and that rule has quietly stopped holding.
- You're using alone, or to take the edge off a regular week, not just to enhance one.
- Your sleep, mood, or memory hasn't felt right for months.
- You've tried to cut back and couldn't, or you cut back and felt worse than you expected.
- You're spending money you don't have, or keeping use secret from people who used to know everything about you.
NIDA describes this pattern clearly: tolerance, withdrawal-like aftereffects, and continued use despite knowing it's causing harm 4. If two or three of those sentences made your stomach drop, that is useful information, not a verdict. It means an honest assessment with a clinician is worth your time, and you have not waited too long.
Matching Care to What You Actually Need
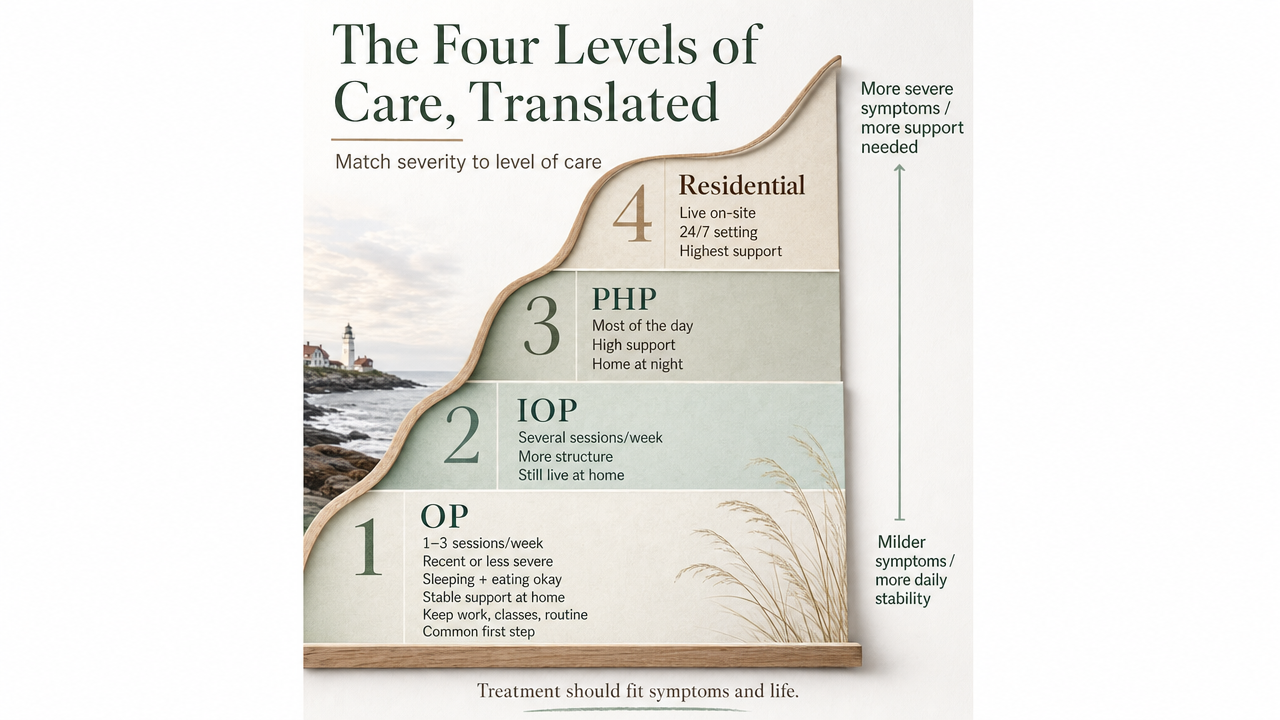
The Four Levels of Care, Translated
When people picture "rehab," they usually picture a 30-day residential stay with their phone taken away. That is one option. It is rarely the right starting point for MDMA use, and it is almost never the only option. SAMHSA's framing is that treatment should be individualized and whole-patient, combining therapy with whatever medical or medication support a person actually needs 1. In practice, that means matching the level of care to your symptoms and your life, not to a brochure.
Here is the ladder, in plain language:
- Standard Outpatient (OP).
- One to a few therapy sessions a week, usually evenings or before work. Good fit when use is recent or less severe, you are sleeping and eating, and you have stable support at home. You keep your job, your classes, your routine. This is where many first-time treatment seekers start.
- Intensive Outpatient (IOP).
- Roughly nine to twelve hours a week of structured group and individual therapy, often three days a week with morning, afternoon, or evening tracks. Good fit when use is weekly or escalating, when mood, sleep, or anxiety has been off for months, or when you have tried to cut back on your own and it has not held. You still go home each night.
- Partial Hospitalization (PHP).
- A daytime program, usually five days a week for several hours a day. Good fit when symptoms are heavier, when polysubstance use is in the picture, or when you are stepping down from a hospital stay and need more structure than IOP can hold.
- Emergency Department or medical evaluation.
- Not a level of "rehab" at all, but the right first stop when there are physical red flags from MDMA use itself, including very high body temperature, confusion, chest pain, seizures, or signs of serotonin syndrome 6. Get medically cleared first. Treatment planning comes after you are safe.
You do not have to know which tier is yours. A clinical assessment sorts that out in one conversation.
When the Emergency Room Comes First
Most people reading this do not need an ER. But it is worth knowing the line, because MDMA can put you over it faster than other party drugs, especially when it is mixed with alcohol, stimulants, or whatever else was around that night.
This is not about overreacting. It is about the right tool for the right moment. An ER stabilizes the body. It does not treat the use disorder underneath. Once you are medically cleared, the next conversation, ideally before you leave the hospital, is what outpatient care looks like from here. A social worker or care coordinator can help you set that up so you are not walking out the door with a discharge paper and no plan.
What Behavioral Treatment Actually Looks Like
The Therapies That Do the Real Work
When you walk into an outpatient program, you are not getting a lecture about drugs. You are getting a handful of specific tools that, used together over weeks, change how you respond to the moments that used to end with you texting your dealer.
Cognitive Behavioral Therapy (CBT). This is the one most people have heard of. You and a therapist map the chain that leads to use: the trigger (a Friday text, a stressful shift, a specific friend group), the thought ("one night won't matter"), the feeling, the action. Then you build different responses for each link. It sounds simple. It works because you practice it on real Tuesdays, not in theory.
Dialectical Behavior Therapy (DBT). Originally built for people who feel emotions at high volume, DBT teaches four skill sets: distress tolerance, emotion regulation, mindfulness, and interpersonal effectiveness. If your MDMA use is partly about turning the volume down on anxiety or numbing out after fights, DBT gives you ways to do that without the drug.
Motivational Interviewing. Less about techniques, more about how the conversation feels. A good clinician will not argue you into quitting. They will help you hear your own reasons out loud, including the ones you've been avoiding.
Relapse Prevention. A specific track, usually woven into the others, that names your personal high-risk situations and rehearses what you do instead. SAMHSA describes this whole-patient approach as the foundation of evidence-based substance use care 1.
Group sessions add something individual therapy can't: hearing someone else describe your Tuesday and realizing you are not the only one.
Why There's No Pill for MDMA Use Disorder
For opioids, there are medications like buprenorphine and naltrexone. For alcohol, there are several. For MDMA, there is nothing on that list. No FDA-approved medication exists specifically for MDMA use disorder, and the research community has been honest about that gap 4, 9.
Part of the reason is how MDMA acts on the brain. It floods the serotonin system rather than locking onto a single receptor the way opioids do, which makes a clean pharmacological target harder to design. Part of it is that MDMA dependence patterns, while real, look different from opioid or alcohol dependence, so the same medication playbook does not transfer.
What this means for you: medication still has a role, just not as a direct MDMA blocker. If you're also dealing with alcohol use, depression, anxiety, sleep problems, or ADHD, medication-assisted treatment for those specific conditions can take real weight off the recovery work 1. The behavioral therapies do the lifting on the MDMA piece. Medication, when it fits, makes the lifting possible.
Treating What MDMA Is Often Covering Up
Anxiety, Depression, Trauma, and the Mood Crash
Ask people why they started using MDMA and you'll hear about fun, music, connection. Ask why they kept using, especially as the hangovers got worse, and the answers shift. "It's the only time I don't feel anxious." "It's the only time I feel close to people." "It quiets the thing in my head I can't quiet on my own."
That is the part of MDMA use that detox cannot touch, because there is nothing to detox in the traditional sense. The work is figuring out what the drug was doing for you, and finding something else that can do that job without the Tuesday cost.
For a lot of people, what surfaces underneath is anxiety, depression, or unprocessed trauma. NIDA notes that the days after use often bring confusion, depression, sleep problems, and trouble with attention and memory, and for heavy users those symptoms can linger 5. If you were already carrying low-grade depression or panic before you started using, MDMA didn't invent those feelings. It muted them temporarily, then made them louder on the back end.
A trauma-informed outpatient program treats both layers at once. You get behavioral therapy for the use itself, and you get real mental health care, sometimes medication for the depression or anxiety, sometimes EMDR or trauma-focused CBT for what's underneath, sometimes both 1. Treating only the MDMA and ignoring the rest is how people end up back in the same loop six months later.
The Polysubstance Reality
Here's something most MDMA articles tiptoe around: almost nobody uses only MDMA. There's usually alcohol in the night. Often weed. Sometimes ketamine, cocaine, or whatever else was passing around. By morning, a benzo or a sleep aid to come down. By Wednesday, more caffeine than your body knows what to do with. The drug you came in worried about is rarely the whole picture.
The national data backs that up. SAMHSA's 2024 Drug Abuse Warning Network report counted an estimated 8.4 million drug-related emergency department visits in 2024, and 21.3% of them involved more than one substance 3. That is roughly one in five ED visits where a single-drug story didn't fit. Research specifically on MDMA users has shown the same pattern from a different angle: substance use disorders for other drugs are common among people who use MDMA recently 13.
Why does this matter for your treatment plan? Because a program that treats only MDMA and ignores the weekend drinking, the daily weed, or the Adderall you take to function on no sleep will not hold. Recovery from MDMA without addressing the alcohol that always rode shotgun is a half plan. Good outpatient care starts with an honest inventory of everything in the picture, then builds a plan around all of it.
This is also where care coordination earns its keep. Your therapist talking to your prescriber, your prescriber knowing what you're actually using, and someone keeping track of the whole picture so nothing falls through the cracks. SAMHSA's whole-patient framing exists for exactly this reason 1. You are not a single-drug case. Your plan shouldn't be either.

Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
MDMA-Assisted Therapy Is Not Treatment for MDMA Addiction
If you've been reading the news at all, you've seen headlines about MDMA as a breakthrough therapy. That's a real story, and it's worth understanding, because the way it gets reported can leave you thinking the drug that's hurting you is also the cure. It is not.
Here's what the research actually measured. In Phase 3 trials of MDMA-assisted therapy for PTSD, after three carefully supervised sessions, 67% to 71% of participants no longer met diagnostic criteria for PTSD, compared with 32% to 48% in the placebo-assisted therapy group 8. Those are meaningful numbers. They are also numbers about PTSD, not about MDMA use disorder. The participants were people with treatment-resistant trauma symptoms, not people trying to stop using ecstasy on weekends.
Even in the PTSD context, the picture is unsettled. In 2024, an FDA advisory committee voted against approval, citing concerns about blinding, missing safety data, and study conduct 7. The research continues, including a new VA trial enrolling about 80 veterans to compare MDMA-assisted therapy with active placebo psychotherapy for PTSD and alcohol use disorder 15. Important work, still in progress, not a treatment you can sign up for at an outpatient clinic.
There is also an older review asking whether MDMA might help treat substance use disorders directly. It noted possible interest while flagging MDMA's own moderate abuse liability as a serious concern, especially for people with addiction histories 9. Translation: using the drug that's the problem to treat the problem is not where the evidence points.
Building a Recovery Plan That Fits Your Life
Keeping Your Job, School, or Family in the Picture
One of the quiet fears that keeps people stuck is the worry that asking for help means losing everything they've built. The job. The semester. The custody arrangement. The version of yourself your family thinks they know. That fear is doing more damage than the truth would.
Outpatient care is built for exactly this reason. An Intensive Outpatient program runs around nine to twelve hours a week, often in morning, afternoon, or evening tracks, which means you can keep working a full schedule or stay enrolled in classes while you're in treatment. A Partial Hospitalization program is heavier, but it still sends you home at night. SAMHSA's framing is that good care should be individualized and shaped around the whole person, not the other way around 1.
You don't have to tell your boss what kind of treatment you're in. Most employers only need to know you have a recurring medical appointment. The Family and Medical Leave Act exists for situations like this if you need protected time. A care coordinator can help you sequence sessions around shifts and deadlines so you're not choosing between your paycheck and your recovery. That choice is a false one, and the right program will help you stop framing it that way.
Relapse Prevention Without the Pep Talk
Relapse prevention is not a motivational poster. It is a specific, written plan you build with your therapist for the moments your brain will absolutely try to talk you out of the plan.
It starts with naming your high-risk situations honestly. The festival weekend on the calendar. The group chat that lights up on Thursday night. The Tuesday crash you now know to expect. Then you decide, in advance and on paper, what you do instead. Who you call. Where you go. What you say. The point is to move the decision out of the moment, because the moment is where the drug usually wins.
You will also build skills for the slip if it happens. A slip is not a failure of the whole project. It is information. NIDA describes the pattern of continued use despite knowing it causes harm as part of how MDMA dependence actually behaves 4, which is exactly why a serious plan assumes some friction and builds for it instead of pretending the road is straight. Telling one person the truth on a hard night counts. So does showing up to your next session anyway.
Your First Move
Here is the part most articles save for the end and bury in clinical language: you do not have to know what you need before you ask. You just need one phone call, one form, one honest conversation. That is the whole first move.
If you are not ready to commit to a specific program, start with SAMHSA's National Helpline at 1-800-662-HELP (4357). It is free, confidential, and open every hour of every day 2. They will not pressure you. They will help you find local options based on what you describe. You can call before you've told anyone in your life.
If you are ready to talk to a clinician, the next step is a simple assessment. A good outpatient program will sit with you, ask honest questions about your use and your week, and recommend a level of care that fits both your symptoms and your schedule 1. You leave that conversation with a plan, not a sales pitch.
If you are in Maine and want trauma-informed outpatient care that coordinates the whole picture, including any mental health support you might need alongside it, Coastal Recovery Partners is one option worth a call. Wherever you start, the win today is the same: one truthful conversation. That is more than most people do in a year of meaning to.
Frequently Asked Questions
Is there a medication that treats MDMA addiction?
No. There is no FDA-approved medication specifically for MDMA use disorder 4, 9. Treatment relies on behavioral therapies like CBT, DBT, and relapse prevention. Medication can still help if you also have depression, anxiety, sleep problems, or another substance use disorder alongside it, but the MDMA piece itself is treated through structured therapy and mental health support, not a daily pill 1.
Do I need to go to detox or residential rehab to stop using MDMA?
Usually not. MDMA does not require traditional medical detox the way alcohol or opioids do. Most people start with outpatient care, ranging from a few sessions a week to a daytime program, and stay in their homes 1. Residential or emergency care comes in only if there are acute physical symptoms like dangerous body temperature, chest pain, or severe confusion 6.
Can I get treatment for MDMA use while keeping my job or staying in school?
Yes. Intensive Outpatient programs typically run nine to twelve hours a week and offer morning, afternoon, or evening tracks built around work and class schedules 1. You go home each night. Your employer only needs to know you have a recurring medical appointment, not the details. The Family and Medical Leave Act can protect time off if you need it for sessions or assessments.
Is MDMA-assisted therapy a treatment for MDMA addiction?
No. MDMA-assisted therapy is being studied for PTSD, not as a treatment for MDMA use disorder. Phase 3 trials showed 67–71% of PTSD patients no longer met diagnostic criteria after three sessions, versus 32–48% with placebo-assisted therapy 8. The FDA voted against approval in 2024 7, and a new VA trial enrolling about 80 veterans is still in progress 15. Different condition, different research.
How do I know if my MDMA use has become a real problem?
Watch for a few patterns: needing more to feel the same effect, using more often than you planned, trying to cut back and not being able to, and continuing despite knowing it is hurting your sleep, mood, work, or relationships. NIDA describes exactly this pattern of tolerance, withdrawal-like aftereffects, and use despite harm 4. If two or three of those fit, a clinical assessment is worth your time.
What is the first step if I'm not ready to commit to a treatment program?
Call SAMHSA's National Helpline at 1-800-662-HELP (4357). It is free, confidential, and open 24 hours a day, every day of the year 2. You do not have to give your name or sign up for anything. They will listen, ask a few questions, and point you to local options based on what you describe. One phone call. That is the whole first step.
References
- Treatment Options for Substance Use Disorder - SAMHSA. https://www.samhsa.gov/substance-use/treatment/options
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- Drug Abuse Warning Network: National Estimates From Drug-Related Emergency Department Visits, 2024. https://www.samhsa.gov/data/sites/default/files/reports/rpt56252/dawn-national-estimates-2024.pdf
- MDMA (“Ecstasy” or “Molly”). https://nida.nih.gov/sites/default/files/mdma_1.pdf
- MDMA (Ecstasy) Abuse. https://nida.nih.gov/sites/default/files/rrmdma_0.pdf
- 3,4-Methylenedioxymethamphetamine (MDMA) Toxicity. https://www.ncbi.nlm.nih.gov/books/NBK538482/
- MDMA-Assisted Therapy for Post-Traumatic Stress Disorder - PubMed. https://pubmed.ncbi.nlm.nih.gov/39955464/
- MDMA and MDMA-Assisted Therapy - PubMed. https://pubmed.ncbi.nlm.nih.gov/39741438/
- Can MDMA play a role in the treatment of substance abuse? - PubMed. https://pubmed.ncbi.nlm.nih.gov/23627786/
- A Review of 3,4-methylenedioxymethamphetamine (MDMA) - PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6435835/
- The pharmacology and toxicology of “ecstasy” (MDMA) and related drugs. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC81503/
- Ecstasy-Related Emergency Department Visits by Young People Increased Between 2005 and 2011. https://www.samhsa.gov/data/sites/default/files/spot127-youth-ecstasy-2013/spot127-youth-ecstasy-2013.pdf
- The high prevalence of substance use disorders among recent MDMA users. https://pmc.ncbi.nlm.nih.gov/articles/PMC2745898/
- NIDA: Advancing Addiction Science for 50 Years. https://nida.nih.gov/videos/nida-advancing-addiction-science-50-years
- VA launches MDMA-assisted mental health therapy trial - VA News. https://news.va.gov/press-room/va-launches-mdma-assisted-mental-health-therapy-trial/



