
Finding Meth Rehab Near Me: A Step-by-Step Guide

Key Takeaways
- The first hour only requires a private moment, your zip code and insurance info, and one honest call to SAMHSA's helpline at 1-800-662-HELP 7.
- Modern meth rehab is layered behavioral care — contingency management, CBT, and the Matrix Model — not a detox pill or a single 30-day program 1.
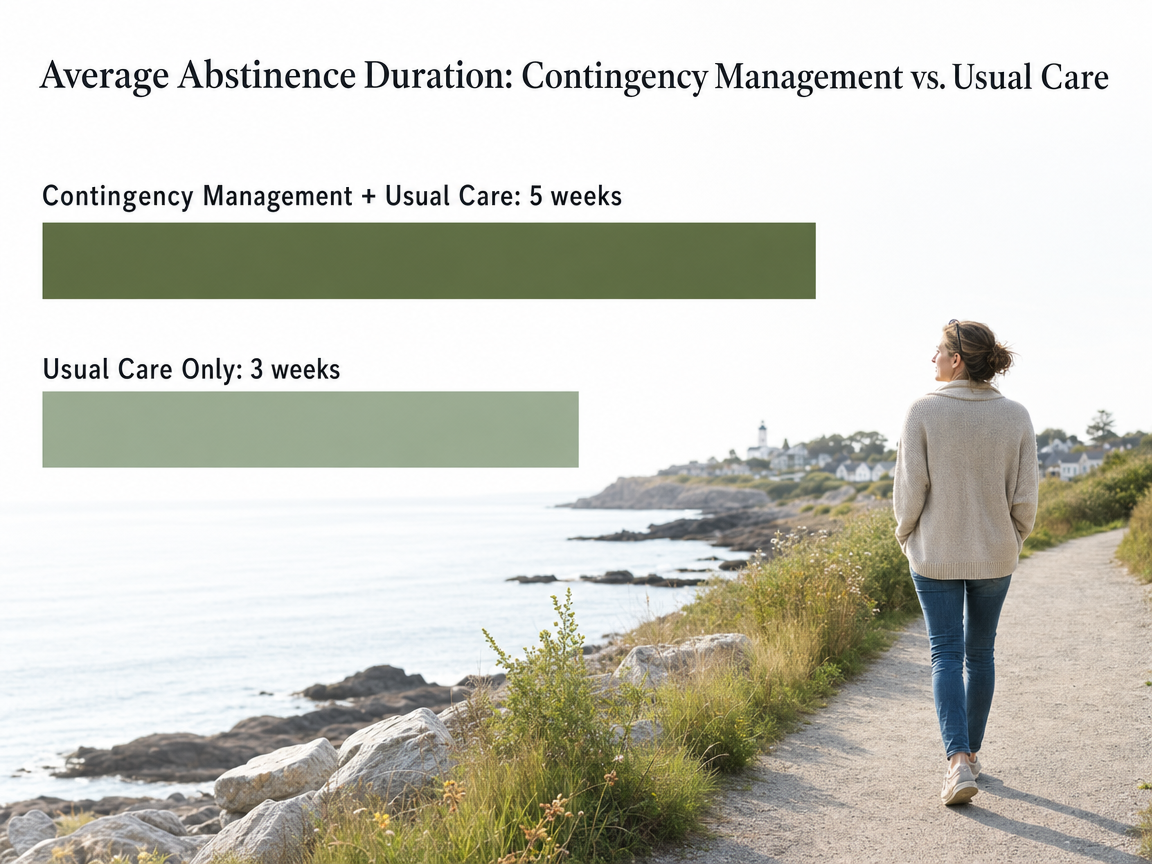
- Contingency management is the evidence-backed core, with one trial showing 5 weeks of continuous abstinence versus 3 weeks for usual care alone 3.
- No FDA-approved medication exists for meth use disorder, though off-label naltrexone plus bupropion showed a 13.6% vs 2.5% response over placebo 15, 4.
- Skip paid search ads and use SAMHSA's helpline, FindTreatment.gov, and Maine's behavioral health directory to find programs without financial conflicts 7, 16.
- On the intake call, ask six specific questions covering contingency management, trauma-informed care, dual diagnosis, medical coordination, scheduling, and aftercare 1.
- Aftercare holds gains by naming specifics — step-down outpatient, alumni groups, relapse prevention, and continued prescriber coordination — before IOP ever ends 17.
Start where you are: the first hour after you decide to look
You decided to look. That itself is the hardest step, and you already took it. Whatever pulled you here — a scary night, a worried text from your sister, the quiet realization at 3 a.m. — the next hour does not have to be perfect. It just has to be honest and small.
Here is what that first hour can hold. Sit somewhere private. Put your phone on silent for everything except the one call you are about to make. Write down three things on paper: your zip code, your insurance card info if you have it, and one sentence about what is going on. That sentence can be as plain as, "I am using meth and I want help," or, "My partner has been using and I do not know what to do." You do not need to perform a crisis. You just need to be able to say the sentence out loud.
Then call SAMHSA's National Helpline at 1-800-662-HELP (4357). It is free, confidential, and open 24/7, in English and Spanish, and the person on the other end will help you find treatment near South Portland without judgment or a sales pitch 7.
That is the first hour. Not a plan for the rest of your life. Just a call, a sentence, and the smallest forward motion. That counts.
What meth rehab actually means in 2025
The phrase "meth rehab" sounds like one thing. It is not. In 2025, treatment for methamphetamine use disorder is a layered approach built around behavioral therapy, with medication and other supports added when they help. There is no detox pill, no week-long fix, and — being straight with you — no medication the FDA has approved specifically for meth use disorder yet 4.
What does work, and what the major clinical guidelines now point to, is structured behavioral care. The ASAM and American Academy of Addiction Psychiatry guideline names contingency management — a method that rewards verified drug-free urine screens with small incentives — as the current standard of care for stimulant use disorders, including meth 1. Around that core, programs layer cognitive behavioral therapy, the Matrix Model (a 16-week outpatient framework designed for stimulants), group sessions, and individual counseling 5.
Most adults do not need a 30-day bed in a residential facility to access any of this. Intensive outpatient programs deliver the same evidence-based therapies in a schedule that lets you sleep at home, keep your job, and see your kids 17. You go to treatment several times a week, in mornings or evenings, and the rest of your life keeps moving.
The other piece that matters in 2025: trauma-informed care and dual diagnosis treatment. Meth use rarely shows up alone. Anxiety, depression, PTSD, ADHD, and past trauma often ride alongside it, and a good program treats those at the same time — not after you "get clean first" 10. That is what modern meth rehab actually is. A schedule, a set of therapies that have evidence behind them, and people who understand that your brain and your story both matter.
Choosing the right level of care for your life
Outpatient, IOP, PHP, or residential: a working adult's decision tree
Here is the part nobody explains clearly: "meth rehab" is not one program. It is a ladder of options, and you pick the rung that matches your life right now. The rungs are usually described as outpatient (OP), intensive outpatient (IOP), partial hospitalization (PHP), and residential. The difference is mostly about how many hours per week you are in treatment and how much of your normal life keeps running alongside it.
Standard outpatient is the lightest touch — usually one to a few hours a week of individual counseling or a single group. It fits people who are stable, working, and either stepping down from a higher level of care or catching things early. Intensive outpatient typically runs around nine to twelve hours a week, often three days of group therapy plus individual sessions, scheduled in mornings or evenings so you can still work or pick up your kids. Partial hospitalization is more intensive — closer to twenty or more hours a week, almost like a part-time job — but you still sleep at home. Residential is 24/7 care in a facility, usually for two to four weeks or longer.
Here is what matters for the choice. A well-structured IOP can be as effective as inpatient treatment for many adults with substance use disorders, especially when home life is reasonably stable and withdrawal is manageable 6. That finding is the reason you do not have to assume residential is automatically "better." For a working parent in South Portland whose mornings belong to school drop-off, an evening IOP often delivers the same evidence-based therapies — CBT, group work, contingency management — without dismantling the rest of your life. Start by asking which level a clinical assessment recommends, then ask why.
When residential is the right call (and when it isn't)
Residential is the right call in specific situations, and being honest about them matters more than defaulting to the most intensive option. If your home is not safe or sober, if you are using daily and have not been able to stop for even a few days on your own, if you have severe co-occurring mental health symptoms that need round-the-clock monitoring, or if past outpatient attempts have not held — residential gives you a reset that outpatient cannot 17.
It is not the right call just because meth feels scarier than other drugs, or because someone told you that "real rehab" means 30 days inland. Many adults with methamphetamine use disorder do better with structured outpatient care that keeps their job, their housing, and their relationships intact. Losing those during a long residential stay can leave you more vulnerable, not less, when you come home.
If you are genuinely unsure, a clinical assessment from an outpatient provider can tell you in one visit whether you can safely start at IOP or PHP, or whether residential makes sense first. You do not have to guess.
What evidence-based meth treatment looks like inside the room
Contingency management, CBT, and the Matrix Model in plain English
If you are going to spend ten or fifteen hours a week in a program, you deserve to know what those hours are supposed to do. Here is the short version of the three approaches you will hear about most often for meth.
Contingency management, or CM, is the one with the strongest evidence and the strangest name. It works like this: when you submit a urine screen that confirms you have not used, you earn a small reward — a gift card, a voucher, a prize draw. That is it. No lecture, no punishment for a positive screen, just a real-world reinforcement for the behavior you are trying to build. It sounds almost too simple, but the data is clear. In one randomized trial, adults with methamphetamine use disorder who received contingency management alongside usual treatment stayed continuously abstinent for an average of 5 weeks, compared with 3 weeks for those getting usual care alone 3. That gap is why the ASAM/AAAP clinical practice guideline now calls contingency management the standard of care for stimulant use disorders 1.
Cognitive behavioral therapy, or CBT, is the talk-therapy half of the equation. You and a counselor map out the thoughts, triggers, and situations that lead to using, then build specific skills to handle them. Systematic reviews of CBT for methamphetamine use find consistent reductions in use even after relatively brief treatment episodes 11.
The Matrix Model pulls it all together. It is a 16-week outpatient framework built specifically for stimulants — group education, individual sessions, family involvement, drug testing, and relapse prevention woven into a single schedule 5. When you hear a program describe itself as Matrix-informed, that is the structure they mean.
Ask programs directly which of these three they offer, and how.
Trauma-informed care and treating what's underneath the use
Meth is rarely the whole story. For most adults in treatment, there is something underneath — old trauma, untreated anxiety or depression, ADHD that nobody named, a grief that never had a place to land. SAMHSA's treatment protocol for stimulant use disorders is explicit that effective programs assess for co-occurring mental health conditions and trauma histories from the start, not after some imagined finish line of "getting clean first" 10.
Trauma-informed care is not a slogan. In practice, it means the staff is trained to recognize how trauma shapes behavior in a group room. It means you are not asked to share your worst memory on day one to prove you are serious. It means physical safety, predictable routines, choice in how you participate, and an awareness that shame is the fastest way to push someone back to using.
Dual diagnosis treatment is the clinical term for treating substance use and mental health together, in the same program, with providers who talk to each other. If a program tells you to get sober and then come back for therapy, that is not dual diagnosis. Keep calling.
The honest truth about medications for meth use disorder
What does exist is promising off-label research. The ADAPT-2 trial tested a combination of extended-release injectable naltrexone plus oral bupropion in adults with moderate to severe meth use disorder. The combination beat placebo — a weighted response rate of 13.6% versus 2.5% over 12 weeks 15. That is real, and it matters, but the absolute response is modest. Medication is a complement to behavioral treatment, not a replacement for it 4.
Two other medication conversations come up in good programs. One is medication-assisted treatment for co-occurring opioid use disorder, which is common when meth and fentanyl get mixed in the same supply. The other is treating the mental health conditions sitting underneath — depression, ADHD, anxiety — with appropriate prescriptions, coordinated with your therapy.
Ask whether a program has a medical director who can prescribe and coordinate these options. That coordination is the point.
Finding programs near South Portland without getting lost in ads
Search "meth rehab near me" and the first page is mostly paid ads, lead-generation sites, and call centers in another state that will route you to whichever facility paid them most that morning. You are not failing at the internet. The internet is doing exactly what it was designed to do. Here is how to step around it.
Start with three sources that do not have a financial stake in where you land. The SAMHSA National Helpline at 1-800-662-HELP (4357) gives you live, confidential referrals to local treatment options, in English or Spanish, any hour of the day 7. SAMHSA also runs FindTreatment.gov, a searchable directory you can filter by zip code, level of care, and insurance. The Maine Office of Behavioral Health and the state's broader substance use response infrastructure publish provider information that is not pay-to-play, and Maine's expansion of medication-assisted treatment and integrated behavioral health care has widened the network of legitimate outpatient providers in the South Portland area over the last several years 16.
Once you have a short list of three or four real programs, look for signals that they actually treat methamphetamine use disorder, not just "all substances" as a marketing line. A legitimate local program will list specific therapies — CBT, contingency management, the Matrix Model — and will name the levels of care they offer in-house, like IOP and PHP. They will have a Maine-based phone number that goes to a clinician or intake coordinator, not a national 800 line. They will tell you their physical address in South Portland or nearby, and they will not pressure you to commit on the first call.
That short list is what you will actually call next.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
The call: a script and the six questions that separate good programs from filler
You have your short list. Now you have to dial. This is the part that makes most people set their phone down three times before they pick it back up. That is normal. Here is exactly what to say so you do not have to improvise while your heart is pounding.
Open with one sentence: "Hi, my name is ___. I'm looking for treatment for methamphetamine use, and I'd like to ask a few questions about your program." That is it. You are not auditioning. You do not owe them your story. If the person who answers cannot answer clinical questions, ask to be transferred to an intake coordinator or clinician.
Then work through these six questions. Write the answers down so you can compare programs later.
- 1. Do you offer contingency management for stimulant use? This is the one the ASAM/AAAP guideline names as the standard of care for stimulant use disorders, including meth 1. Some programs still do not offer it because of funding and regulatory hurdles, so a clear yes or a clear plan to add it tells you a lot 9.
- 2. Is your program trauma-informed, and how does that show up in group? Listen for specifics, not slogans.
- 3. Do you treat co-occurring mental health conditions in the same program, or do you refer out? Same-program dual diagnosis is what you want.
- 4. Do you have a medical director who can coordinate medications? For meth, that may include off-label options or treating an underlying condition.
- 5. What scheduling options do you have — mornings, evenings, multiple tracks? If you work, this question is non-negotiable.
- 6. What does aftercare look like when IOP ends? A real answer names step-down outpatient, alumni groups, or relapse prevention.
You do not need every answer to be perfect. You need enough honest answers to choose.
Insurance, confidentiality, and what missing ten hours a week actually looks like
Three practical worries usually arrive together: Will my insurance cover this? Will anyone find out? And how am I supposed to disappear from work for ten hours a week without raising flags?
On insurance: most legitimate outpatient programs in the South Portland area accept commercial insurance and MaineCare, and they should be able to run a benefits check for you on the first call. Ask what your out-of-pocket cost per week looks like before you commit, and ask whether they offer a sliding scale or care coordination if coverage is thin. Maine has been steadily expanding its behavioral health and medication-assisted treatment infrastructure, which has widened in-network options for outpatient care 16.
On confidentiality: federal law (42 CFR Part 2) protects your substance use treatment records more strictly than general medical records. Your employer cannot pull them. Your family cannot pull them without your written consent. The SAMHSA helpline itself is confidential and does not ask for your name 7.
On the missing hours: a typical IOP runs around nine to twelve hours a week, often split into three evening sessions 17. Many people use existing PTO, FMLA, or a quiet conversation with HR framed as "a health matter." You do not owe anyone the diagnosis. You owe yourself the time.
Your first week, hour by hour
The unknown is half of what makes the first week hard. So here is what it actually looks like, roughly, at a real outpatient program.
- Day one is usually an intake assessment — about ninety minutes with a clinician who asks about your use history, mental health, medical issues, and home situation. They are not trying to catch you. They are trying to match you to the right level of care and build a treatment plan you actually agree with 17.
- Day two or three is often your first group session. You will not be asked to share your life story. Most groups open with a check-in and move into skill-building — handling cravings, identifying triggers, practicing what to say when someone offers you a pipe.
- Later that week, you meet your individual counselor and, if the program offers it, submit your first urine screen as part of contingency management. A negative screen earns a small incentive 3. That is the architecture.
Sleep will be rough. Cravings will spike at strange hours. Show up to the next session anyway. That is the whole job this week.
When the program ends: aftercare that actually holds
Finishing IOP is not the finish line. It is the part where the work changes shape. The early weeks taught you skills in a room with a counselor and a group. Aftercare is where those skills meet a Tuesday night with nothing to do.
A good program plans for that on purpose. Ask, before you ever enroll, what the step-down looks like. The right answer names specifics: a move from IOP into standard outpatient with weekly individual sessions, an alumni group that meets on a consistent night, relapse prevention check-ins, and continued coordination with any prescriber managing depression, anxiety, or co-occurring opioid use 17. If contingency management was part of your IOP, ask how rewards taper without dropping off a cliff 14.
Build in human anchors too. One person you call before you use. One meeting on the calendar each week. One honest sentence ready when someone asks how you are.
You did the hard part. Aftercare is how you keep it.
Frequently Asked Questions
Can I go to meth rehab without taking time off work?
Often, yes. Intensive outpatient programs are built for working adults — typical schedules run around nine to twelve hours a week in morning or evening sessions, so you sleep at home and keep your job 17. Ask about evening tracks specifically when you call, and bring your work hours to the intake assessment.
Is outpatient treatment really enough for meth addiction, or do I need residential?
For many adults, a well-structured IOP can be as effective as inpatient care, especially when home is stable and withdrawal is manageable 6. Residential makes more sense if your living situation is unsafe, you have severe co-occurring mental health symptoms, or outpatient attempts have not held. A clinical assessment will tell you which level fits — you do not have to guess.
Is there a medication that treats methamphetamine use disorder?
Not specifically — the FDA has not approved any medication for meth use disorder yet 4. Some programs use off-label combinations like extended-release naltrexone plus bupropion, which showed a modest but real benefit over placebo in a recent trial 15. Medication can support treatment, but behavioral therapy remains the foundation. Ask whether a program has a medical director who can coordinate options.
What is contingency management, and why should I ask if a program offers it?
Contingency management rewards verified drug-free urine screens with small incentives like gift cards or vouchers. It sounds simple, but the ASAM/AAAP clinical practice guideline names it the current standard of care for stimulant use disorders, including meth 1. Not every local program offers it yet because of funding and regulatory hurdles 9, so a clear yes signals a program keeping up with the evidence.
How do I find a legitimate meth rehab near South Portland without getting funneled into ads?
Skip the paid search results. Start with SAMHSA's National Helpline at 1-800-662-HELP (4357), which gives free, confidential referrals in English or Spanish, any hour 7. FindTreatment.gov lets you filter by zip code and level of care. Maine's behavioral health network has expanded steadily in the South Portland area, so legitimate in-network outpatient options exist locally 16.
Will my employer or family find out if I enter treatment?
Not without your written consent. Federal law (42 CFR Part 2) protects substance use treatment records more strictly than general medical records, so your employer cannot pull them and your family cannot access them unless you sign a release. The SAMHSA helpline itself does not ask for your name 7. If you use FMLA or PTO, you owe HR a health reason, not a diagnosis.
References
- The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. https://pubmed.ncbi.nlm.nih.gov/38669101/
- Contingency Management for the Treatment of Substance Use Disorders. https://aspe.hhs.gov/sites/default/files/documents/a0cc6fcdb2968be95f60bb1c2c94eb70/contingency-management-sub-treatment.pdf
- Contingency management for the treatment of methamphetamine abuse. https://pubmed.ncbi.nlm.nih.gov/17074952/
- Combination treatment for methamphetamine use disorder shows promise in NIH study. https://www.nih.gov/news-events/news-releases/combination-treatment-methamphetamine-use-disorder-shows-promise-nih-study
- Current and Emerging Treatments for Methamphetamine Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC9185770/
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Treatment of Stimulant Use Disorders: SAMHSA Evidence-Based Resource. https://integrationacademy.ahrq.gov/news-and-events/news/treatment-stimulant-use-disorders-samhsa-evidence-based-resource
- Barriers to Effective Implementation of Contingency Management in Methamphetamine Treatment. https://scholarworks.seattleu.edu/cgi/viewcontent.cgi?article=1023&context=dnp-projects
- Treatment for Stimulant Use Disorders (TIP Series). https://www.ncbi.nlm.nih.gov/books/NBK576541/
- A systematic review of cognitive and/or behavioural therapies for methamphetamine use. https://pmc.ncbi.nlm.nih.gov/articles/PMC4445690/
- ONDCP Methamphetamine Plan Implementation Report. https://www.whitehouse.gov/wp-content/uploads/2025/03/ONDCP-2024-Methamphetamine-Implementation-Report.pdf
- The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. http://stacks.cdc.gov/view/cdc/156927
- Lessons learned from statewide contingency management rollouts for stimulant use disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC10787039/
- Bupropion and Naltrexone in Methamphetamine Use Disorder. https://pubmed.ncbi.nlm.nih.gov/33497547/
- Opioid Response | Office of Policy Innovation & Future - Maine.gov. http://www.maine.gov/future/opioids
- Intensive Outpatient Treatment Approaches (TIP 47). https://www.ncbi.nlm.nih.gov/books/NBK424859/



