
Choosing Substance Abuse Treatment Models That Fit Your Life

Key Takeaways
- Treatment runs along a continuum from weekly therapy to 24-hour residential care, so the real question is what level of structure fits your life right now.
- Standard outpatient, IOP, PHP, and residential differ mainly in weekly hours and supervision, and people commonly move between levels as their needs shift 16.
- Six signals — withdrawal risk, available hours, co-occurring mental health needs, MAT considerations, home stability, and transportation — help point you toward the right starting level 17, 12.
- Medication-assisted treatment with buprenorphine, methadone, naltrexone, or acamprosate is first-line care that works in outpatient settings alongside counseling, not a last resort 3, 2.
- When mental health and substance use overlap, integrated same-team care produces better engagement and outcomes than sending you between disconnected providers 8.
- Trauma-informed care should show up in screening, staff training, and client choice — ask specific questions instead of trusting the label on a brochure 20.
- Telehealth and hybrid attendance are as effective as in-person care for many people and can hold you through scheduling disruptions that would otherwise end treatment 6, 7.
Treatment is a spectrum, not a single building you check into
If you've spent any time searching for help with drinking, pills, or other substances, you've probably noticed something strange: most of what you read sounds like there are only two doors. Either you keep doing what you're doing, or you pack a bag for 30 days at a residential facility somewhere with a winding driveway and a lake.
That picture isn't accurate, and it isn't fair to you.
Substance use treatment is actually a continuum. It runs from a once-a-week therapy appointment, to intensive outpatient programs that meet several evenings a week, to partial hospitalization that looks more like a full workday, all the way up to 24-hour residential care. The National Institute on Alcohol Abuse and Alcoholism states that people often think the only options are AA or rehab, when in reality there are far more choices than most folks expect, including counselors' offices, clinics, intensive outpatient settings, and primary care practices with medication support 1.
Here's what that means for you. The question isn't "am I sick enough for rehab?" It's "what level of structure do I need right now, and how do I get it without losing the parts of my life worth protecting?" Your job, your kids, your lease, your dog, your morning routine — those aren't obstacles to recovery. For many people, they're reasons recovery sticks.
The rest of this guide walks you through the actual models, the signals that point to each one, and the questions worth asking before you commit to a schedule. Take it one section at a time.
The four main levels of care, in plain language
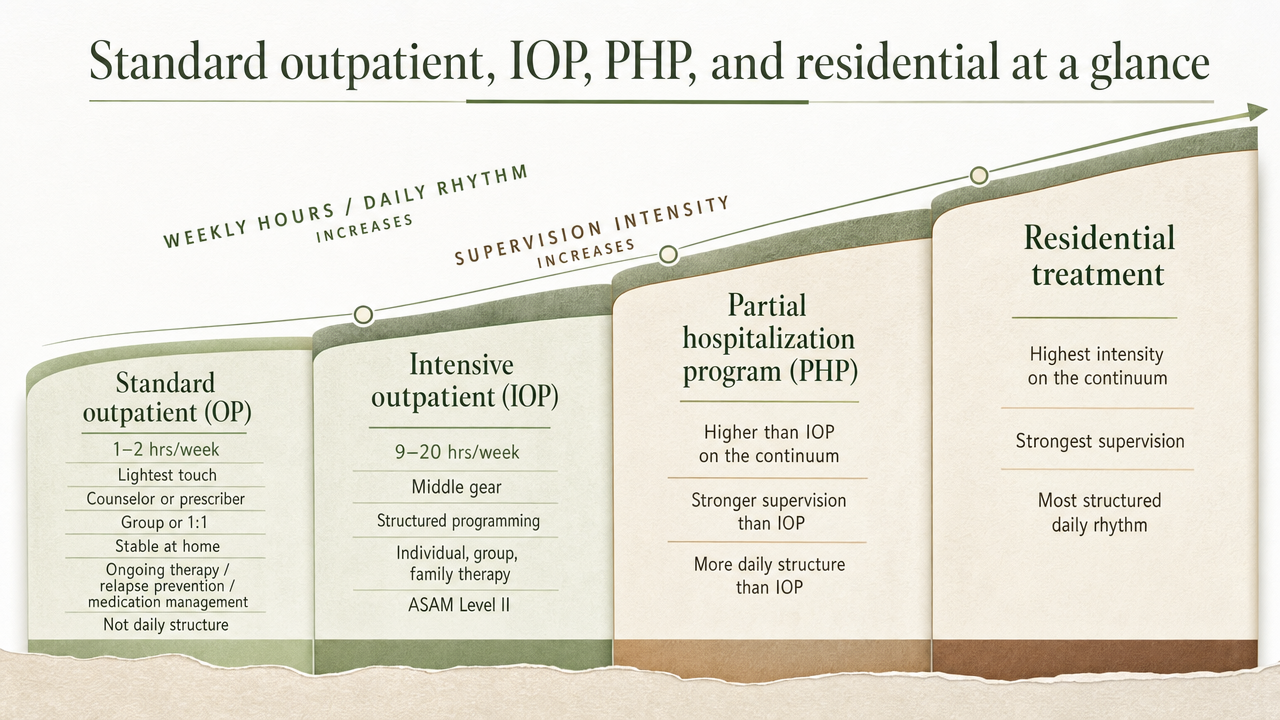
Standard outpatient, IOP, PHP, and residential at a glance
Before you can pick a model, you need a clear picture of what each one actually involves. The names sound interchangeable in marketing copy, but the weekly hours, supervision, and daily rhythm are very different.
Standard outpatient (OP) is the lightest touch. You're usually meeting with a counselor or prescriber for one to two hours a week, sometimes in a group, sometimes one-on-one. It fits people who are stable, have solid support at home, and need ongoing therapy, relapse prevention, or medication management — not a structured daily program.
Intensive outpatient (IOP) is the middle gear. The federal Treatment Improvement Protocol describes IOP as ASAM Level II care that provides structured programming for 9 to 20 hours per week through individual, group, and family therapy 16. Medicare's own coverage rules use that same floor: a person's plan must call for at least 9 hours of therapeutic services each week to qualify 14. Most IOPs run three to five days a week in three-hour blocks, with morning, afternoon, or evening tracks so you can keep a job or get kids to school.
Partial hospitalization (PHP) is more like a full workday of treatment. You're typically there five days a week, often around 20 or more hours, with closer clinical oversight and more medical support than IOP — but you still sleep at home. It's the step many people use when they need real structure but don't need someone watching them around the clock 16.
Residential is 24/7 care in a live-in setting. It exists for situations where home isn't safe to recover in, withdrawal needs medical monitoring, or someone has tried lower levels and needs a full reset.
One thing worth knowing: people often move between these levels 16. You might start in PHP for a few weeks, step down to IOP as you stabilize, and end up in standard outpatient with monthly check-ins. The point isn't to land in the "right" tier on day one. It's to match the structure to where you are this month — and adjust as your life and your recovery change.
What the evidence says about IOP vs. inpatient outcomes
Here's the part most articles bury or skip entirely: for many adults, you don't have to choose between strong treatment and staying in your life. The research backs that up.
A systematic review published in Psychiatric Services looked at the available studies on substance abuse intensive outpatient programs — including PHP and day treatment — and compared them to inpatient and residential care. The authors concluded that IOPs are as effective as inpatient treatment for most individuals who seek care, measured by reductions in substance use and improvements in related life outcomes 15.
The scope here matters, and the reviewers were honest about it. "Most individuals" is not "everyone." The studies they pooled covered adults who were clinically appropriate for outpatient care in the first place — meaning they didn't need medical detox or 24-hour supervision to be safe. Programs differed in hours, therapies used, and how MAT was integrated, so results varied by how well-structured the program was 15. A loosely run IOP is not the same product as a well-staffed one using evidence-based therapies.
What that means for your decision: if a clinician tells you IOP or PHP is a reasonable starting point, that recommendation isn't a downgrade or a budget compromise. It's grounded in the same outcome literature that supports residential care. The questions worth asking shift from "is this enough?" to "is this program well-built?" — meaning, does it use therapies like CBT and motivational interviewing, integrate medication when appropriate, screen for trauma and co-occurring conditions, and coordinate with your other providers? Those program features matter more than the building you walk into.
If your situation includes serious withdrawal risk, an unsafe home, or repeated failed attempts at lower levels of care, residential is still the right call. The evidence isn't telling you to skip a level you need. It's telling you that if outpatient is clinically appropriate, you can take it seriously.
Six signals that point you to the right level of care
You don't need to guess your way through this. There are six practical signals that clinicians actually weigh when they recommend a level of care — and you can think through most of them on your own before you ever pick up the phone. NIDA's core treatment principles back this up: no single approach fits everyone, and matching the setting and services to your specific needs is what makes treatment work 17.
- Withdrawal risk. If stopping alcohol, benzos, or opioids on your own could land you in a medical crisis — shakes, seizures, dangerous blood pressure spikes, severe opioid withdrawal — you need medical supervision before you start any outpatient program. That points to a PHP with medical oversight, a detox setting first, or residential care. If your use is problematic but your body isn't physically dependent, an IOP or standard outpatient program can be a reasonable starting place.
- Hours you can realistically commit. Be honest with yourself. Standard OP asks for one to two hours a week. IOP requires at least nine hours per week and often runs up to twenty 16. PHP eats most of a workday, five days a week. If you can carve out three evenings a week but not five full days, an evening IOP track is a real fit — not a compromise.
- Co-occurring mental health needs. If anxiety, depression, PTSD, or bipolar symptoms are tangled up with your substance use, you need a program built to treat both at once rather than two disconnected providers passing notes. We'll get into what that looks like in a moment.
- MAT considerations. If you're dealing with opioid or alcohol use disorder, medication can change the math on which level of care you need. Buprenorphine, naltrexone, methadone, acamprosate — these aren't reserved for residential settings. They work in flexible outpatient programs when paired with counseling 17.
- Home stability. Recovery is hard if you're going back to a house where substances are around, where someone is using actively, or where you don't feel safe. A stable home raises what outpatient care can do for you. An unsafe home pushes you toward PHP, residential, or sober living alongside outpatient treatment.
- Transportation and logistics. This sounds small until it isn't. A scoping review found that transportation barriers measurably reduce attendance and engagement in outpatient SUD and mental health care, especially in rural or lower-income areas 12. If you don't have a reliable ride at 6 p.m. three nights a week, you need a program close to home, on a bus line, or one that offers telehealth sessions as part of the mix.
Run yourself through these six. If most of your answers point to outpatient territory, that's likely where you start. If two or three point higher, bring that list to an assessment call and let a clinician help you sort the rest.
Medication-assisted treatment belongs in this conversation
If you're weighing options for opioid or alcohol use disorder and no one has brought up medication yet, that's a gap worth closing. MAT — medication-assisted treatment — pairs an FDA-approved medication with counseling to reduce cravings, blunt withdrawal, and keep you steady enough to do the rest of the work.
For opioid use disorder, the 2024 national practice guideline update is clear: buprenorphine, methadone, and extended-release naltrexone are first-line treatments and should be available across office-based, outpatient, and more intensive settings 3. The CDC frames these medications the same way — standard of care when combined with counseling and behavioral therapy, not a last resort 18. For alcohol use disorder, the American Psychiatric Association's guideline recommends offering naltrexone, acamprosate, or disulfiram to appropriate patients alongside psychosocial care 2. NIAAA points out that these alcohol medications are effective and underused — many people who could benefit never get offered them 19.
A few things worth knowing as you think about MAT and which level of care fits you:
You don't need to be in residential to start. A practical guide for primary care clinics shows MAT can be launched in office-based settings, with staffing and workflows built around outpatient care 4. IOP and PHP programs that integrate MAT do the same thing — medication, therapy, and case management under one roof, on a schedule you can keep.
MAT isn't "trading one drug for another." That phrase still circulates, and it's wrong on the science. These medications are dosed and monitored to reduce cravings and the euphoria of misuse so you can function, work, parent, and engage in therapy 18. Stopping them is a clinical decision made with your prescriber, not a moral test you pass.
If medication might be part of your plan, ask any program you're considering whether they prescribe MAT in-house or coordinate with a prescriber, and how medication visits fit into the weekly schedule. That answer tells you a lot about how seriously the program takes the evidence.
When mental health and substance use travel together
For a lot of people, substance use isn't the whole story. There's anxiety underneath the drinking, or depression that the pills used to quiet, or PTSD that nobody ever named out loud. If that sounds familiar, you're not unusual — you're the norm. Substance use disorders are highly comorbid with mood, anxiety, and personality disorders, and treating one without the other tends to leave people stuck 8.
The term you'll hear is dual diagnosis or co-occurring disorders. What it should mean, in practice, is that one team handles both — not two clinics emailing each other once a month. Research on integrated treatment shows that coordinated, same-roof care is associated with better engagement and outcomes than parallel or sequential approaches, where people get sent from a mental health provider to a substance use provider and back again 8. NIDA's core principles say the same thing in plainer language: effective treatment addresses your multiple needs at once, not just the substance use 17.
So when you're evaluating an outpatient or IOP program, ask directly: who handles my anxiety or depression here? Is there a prescriber on staff who can manage psychiatric medications? Will my therapist and my prescriber actually talk to each other, or am I the messenger? Coordinated care isn't a luxury feature. The IOM has flagged for years that coordination prevents drug interactions, redundant appointments, and the kind of dropped handoffs that quietly end recoveries 9.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Trauma-informed care: what to actually ask a provider
Trauma-informed care gets used as a marketing phrase a lot. It shouldn't be. SAMHSA defines it through what it actually does in a program: staff realize the widespread impact of trauma, recognize the signs in clients, respond by building that knowledge into everyday policies and practices, and actively work to resist re-traumatization — the Four Rs 20. Six principles back that up: safety, trustworthiness, peer support, collaboration, empowerment, and attention to cultural and gender issues 20.
Why this matters for you: trauma is common among people with substance use disorders, and care that ignores it tends to lose people early 11. A program that screens for trauma, paces sessions thoughtfully, and gives you real choices in your own treatment is more likely to keep you engaged long enough for the work to land 10.
When you call a program, you can ask specific questions instead of taking the label at face value:
- How do you screen for trauma at intake, and what happens with what I share?
- Are all staff — not just therapists — trained in trauma-informed practices?
- What choices do I have about groups, topics, or activities that feel unsafe?
- How do you handle moments when someone gets triggered in a session?
Clear answers signal a program that lives the principles. Vague ones tell you something too.
Telehealth, hybrid attendance, and the messy middle
Life doesn't pause for a treatment schedule. A kid gets sick. Your shift changes. The car breaks down the same week you finally felt ready to start. This is the part most program brochures gloss over, and it's where a lot of people quietly drop out.
Telehealth has changed what's possible here, and the evidence is solid. A systematic review of telemedicine for substance use disorders found it was as effective as in-person care for reducing substance use and keeping people in treatment 6. A separate review of telehealth SUD services during COVID-19 reached similar conclusions on feasibility and outcomes 5. And on the medication side, NIDA reported on Medicaid data showing that starting buprenorphine through telehealth was linked to better retention than non-telehealth starts 7— a meaningful finding if transportation, childcare, or a rigid work schedule has been the thing keeping you from showing up.
What this looks like in practice: a hybrid week where you attend group in person two evenings, do an individual therapy session by video on your lunch break, and meet your prescriber online for a MAT check-in. You're still in the program. You're just not losing a recovery week to a flat tire.
A few honest caveats. Telehealth isn't right for everyone or every moment. Early stabilization, acute crisis, and some group work land better face-to-face. Privacy at home matters — if there's nowhere quiet to take a session, that's something to solve with your care team, not push through. And technology access is real; not every household has reliable broadband or a private device.
If you're weighing programs, ask which sessions can shift to video when life gets in the way, and what happens if you miss a week instead of two days. The answer tells you whether the program is built to hold you through the messy middle or quietly write you off when you stumble.
What insurance and weekly hours actually look like
Money and hours are usually the two questions running in the background while you read everything else. Let's put real numbers on them.
On the hours side, intensive outpatient programs typically run 9 to 20 hours a week, delivered through group, individual, and family therapy in three- to four-hour blocks 16. Medicare's coverage rules treat 9 hours per week as the floor — your plan of care must call for at least that much therapeutic service for IOP coverage to apply 14. PHP sits above that, usually around 20 or more hours across five days. Standard outpatient is one to two hours a week, sometimes less once you're stable.
On the insurance side, Medicare covers IOP for substance use disorders without requiring you to qualify for inpatient care first 14. Most commercial plans cover outpatient SUD care at varying levels — co-pays, deductibles, and prior authorization rules differ a lot. You don't have to figure this out alone. A care coordinator can verify your benefits, explain what's covered before you start, and flag any authorization steps so a billing surprise doesn't end your treatment two weeks in.
What a care coordination conversation sounds like
If you've read this far and you're still not sure which level fits, that's actually the right place to be. The next step isn't picking a program. It's a phone call.
A care coordination conversation usually runs 20 to 30 minutes. Someone asks about your use, your history, your work schedule, your home, your insurance, and what you've tried before. They're not gatekeeping. They're matching you to a level of care and screening for things that change the plan — withdrawal risk, co-occurring anxiety or depression, whether MAT belongs in the conversation, whether a prescriber needs to be looped in early 9, 17.
You walk away with a few concrete things: a recommended starting level (OP, IOP, or PHP), a sense of what your insurance will cover, a schedule that fits your week, and a short list of next steps. If you have other providers — a therapist, a primary care doctor, a psychiatrist — coordination means your new team talks to them, not that you carry messages back and forth 9.
In Southern Maine, Coastal Recovery Partners offers that kind of recovery planning and care coordination as a starting point, no commitment required. One call. That's the win for today.
Frequently Asked Questions
Do I have to quit my job or leave my family to get real treatment?
No. For most adults who are clinically appropriate for outpatient care, you can keep working and keep showing up at home while you get help. NIAAA points out that treatment happens in clinics, counselors' offices, and intensive outpatient programs — not just inpatient settings 1. Evening and morning IOP tracks exist specifically so a job and a recovery plan can share the same week.
What's the actual difference between IOP and PHP?
Hours and intensity. IOP runs roughly 9 to 20 hours a week, usually three to five days, through group, individual, and family therapy 16. PHP is closer to a full workday, typically around 20 or more hours across five days, with more clinical oversight 16. Both let you sleep at home. PHP fits when you need heavier structure; IOP fits when you can hold a routine with strong weekly support.
Is medication-assisted treatment just trading one drug for another?
No, and the science is clear on this. CDC describes MAT medications like buprenorphine, methadone, and naltrexone as standard of care that reduce cravings and the euphoria of misuse when paired with counseling 18. The 2024 national opioid use disorder guideline treats them as first-line options across outpatient and office-based settings 3. They help you function — work, parent, do the therapy work — not get high.
Will insurance cover outpatient or intensive outpatient care?
Usually, yes. Medicare covers IOP services for substance use disorders when your plan of care calls for at least 9 hours of therapeutic services per week, and you don't have to qualify for inpatient first 14. Most commercial plans cover OP and IOP, though co-pays, deductibles, and prior authorization rules vary. A care coordinator can verify your benefits before you start so the math is clear.
Can I do part of my treatment through telehealth?
Often, yes. A systematic review found telemedicine for substance use disorders is as effective as in-person care for reducing use and keeping people in treatment 6. NIDA also reported that starting buprenorphine through telehealth was linked to better retention than non-telehealth starts 7. Many programs blend in-person group with video individual sessions or MAT check-ins. Ask which sessions can shift to video when your week gets complicated.
What if I have anxiety, depression, or past trauma alongside substance use?
That's common, not disqualifying. Substance use disorders frequently travel with mood, anxiety, and trauma-related conditions, and integrated treatment — one team handling both — is associated with better engagement and outcomes than parallel care 8. Look for a program that screens for trauma at intake and follows SAMHSA's trauma-informed principles of safety, trustworthiness, and collaboration 20. Ask directly how your therapist and prescriber coordinate.
References
- What Types of Alcohol Treatment Are Available?. https://alcoholtreatment.niaaa.nih.gov/what-to-know/types-of-alcohol-treatment
- The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. https://pubmed.ncbi.nlm.nih.gov/29301420/
- Management of opioid use disorder: 2024 update to the national practice guideline. https://pmc.ncbi.nlm.nih.gov/articles/PMC11573384/
- Launching a Medication-Assisted Treatment in an Outpatient Office-Based Practice. https://pmc.ncbi.nlm.nih.gov/articles/PMC7350034/
- Telehealth Services for Substance Use Disorders During the COVID-19 Pandemic: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC8923149/
- Telemedicine-delivered treatment for substance use disorder: A systematic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC11444076/
- Telehealth supports retention in treatment for opioid use disorder. https://nida.nih.gov/news-events/news-releases/2023/10/telehealth-supports-retention-in-treatment-for-opioid-use-disorder
- Integrated Treatment of Substance Use and Psychiatric Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC3753025/
- Coordinating Care for Better Mental, Substance-Use, and General Health. https://www.ncbi.nlm.nih.gov/books/NBK19833/
- Trauma-Informed Approaches and Programs. https://www.samhsa.gov/mental-health/trauma-violence/trauma-informed-approaches-programs
- Trauma-informed Substance Use Treatment. https://cthc.ucsf.edu/trauma-informed-substance-use-treatment/
- Transportation barriers for substance abuse and mental health outpatient treatment programs: A scoping review. https://mavmatrix.uta.edu/socialwork_theses/172/
- Clients' Experiences and Satisfaction with an Integrated Intensive Program for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC11898248/
- Intensive Outpatient Program Services | Medicare Coverage. https://www.medicare.gov/coverage/mental-health-care-outpatient-intensive-outpatient-program-services
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- NIDA Treatment Guidelines (Module on Treatment of Substance Use Disorders). https://webcampus.med.drexel.edu/nida/module_1/content/5_0_Treatment.htm
- Medication-Assisted Treatment for Opioid Use Disorder. https://www.cdc.gov/overdose-resources/search/pages/2019-133.html
- Treatment for Alcohol Problems: Finding and Getting Help. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
- "Focal Point" SAMHSA's Concept of Trauma and Guidance for a Trauma-Informed Approach. https://www.pathwaysrtc.pdx.edu/focal-point-S1510



