
How to Find the Right Alcohol Treatment Programs Near Me

Key Takeaways
- Reframe the search from 'what's closest' to 'what actually fits my life and is strong enough to work,' since good treatment matches the person rather than the reverse 1.
- Use the six ASAM dimensions — withdrawal risk, medical issues, mental health, readiness, relapse history, and home environment — to gauge honestly which level of care matches your situation 6.
- Learn the continuum in plain terms: standard outpatient runs 1–2 hours weekly, IOP 9–20 hours, PHP 20+ hours, and residential means living onsite — higher isn't better, just more support 4.
- Take IOP seriously, because peer-reviewed evidence shows intensive outpatient is as effective as inpatient for reducing alcohol and drug use in most adults while they keep working and living at home 7.
- Verify any program is licensed by Maine DHHS and staffed by credentialed clinicians, and cross-reference through the Maine Office of Behavioral Health before committing 10, 8.
- Confirm the program names specific evidence-based therapies like CBT, DBT, motivational interviewing, and trauma-informed care rather than describing its approach only in feelings-words 5.
- Ask directly about FDA-approved medications for alcohol use disorder — naltrexone, acamprosate, disulfiram — since guidelines recommend them but many programs still underuse them 9, 5.
- If anxiety, depression, or trauma are part of the picture, choose integrated dual-diagnosis care where one team treats both together, which is linked to better engagement and outcomes 3.
Start with the question behind the search
If you typed "alcohol treatment programs near me" into a search bar tonight, you already did something hard. That search isn't casual. It usually happens after a rough morning, a worried text from someone you love, or a quiet moment when you finally admitted to yourself that cutting back on your own hasn't worked. Take a breath. You're in the right place to think clearly for a few minutes.
Here's the thing most articles skip: the real question underneath your search isn't "what's closest to my zip code?" It's something more like, "What kind of help will actually fit my life — my job, my kids, my insurance, the parts of me I haven't told anyone about — and still be strong enough to work?"
That's a better question, and it has a real answer. National guidance from the NIAAA is direct about it: there is no one-size-fits-all solution, and good treatment matches the person, not the other way around 1. You also have every right to be an active participant in that match. Research on shared decision-making in substance use care shows that most people want to be involved in choosing their treatment, and that involvement tends to help 2.
So before you start comparing programs, let's reframe what you're really looking for.
What 'right' actually means in alcohol treatment
"Right" in this context isn't a vibe or a five-star rating. It's a match — between how much support you actually need and what a program is built to deliver. Clinicians have a structured way to figure that out, and you can borrow their thinking before you ever pick up the phone.
The most widely used framework, often called the ASAM criteria, looks at six dimensions of your situation to decide what level of care fits 6. You don't need to memorize the clinical language. You just need to think honestly about six plain-language questions:
- Withdrawal risk: When you stop drinking for a day or two, does your body shake, sweat, or get dangerously anxious? Have you ever had a seizure or hallucination during a break from alcohol?
- Other medical stuff: Are there physical health issues — liver, blood pressure, pregnancy, chronic pain — that need a doctor in the room?
- Emotions and mental health: Are anxiety, depression, trauma, or thoughts of self-harm part of the picture right now?
- Readiness to change: Are you all-in, on the fence, or being nudged here by someone else? All of those are okay — but they point to different kinds of support.
- Relapse potential: How quickly do you tend to slip back when life gets stressful? Have past attempts to cut back unraveled fast?
- Your recovery environment: Is home safe and supportive, or full of triggers? Do you have a job, kids, a sponsor, a sober friend, transportation?
If most of your answers point to mild-to-moderate risk and a workable home life, a high-quality outpatient or intensive outpatient program is often a strong fit. If withdrawal is dangerous or home isn't safe, you likely need something more intensive first. "Right" simply means the level of care meets you where you actually are — not where you wish you were, and not where stigma says you should be.
The levels of care, in plain English
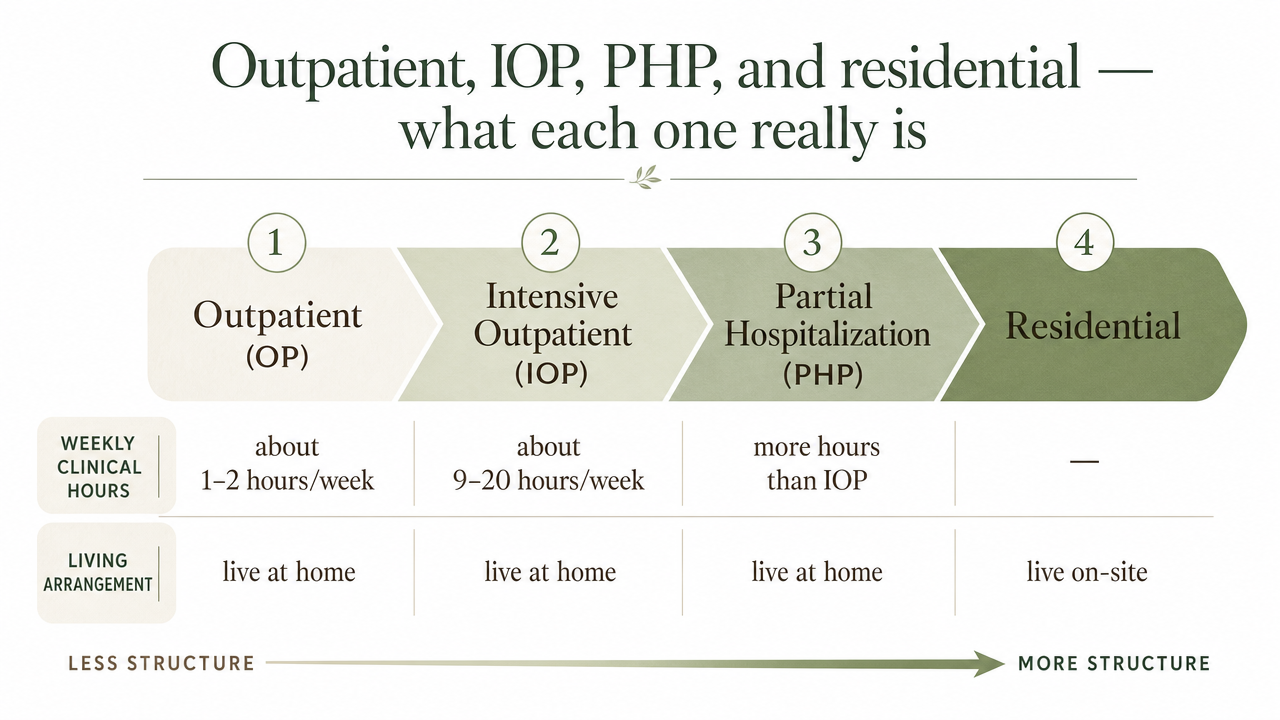
Outpatient, IOP, PHP, and residential — what each one really is
The treatment world has its own alphabet soup, and nobody hands you a decoder ring when you start searching. Here's what the main options actually mean in practical terms, and how clinicians think about where each one fits on the continuum of care 4.
- Standard outpatient (OP)
- The lightest touch — usually about one to two hours a week of individual or group therapy. It works well when your drinking is more contained, your home life is stable, and you mostly need a skilled therapist to help you keep building on progress you've already started.
- Intensive outpatient (IOP)
- The middle gear, and it's where a lot of working adults land. You're typically in clinical programming around 9 to 20 hours a week, often spread across three to five days, with morning or evening tracks so you can keep working. IOP gives you real structure — group therapy, individual sessions, skill-building, often medication support — without sending you away from home 4.
- Partial hospitalization (PHP)
- The most intensive outpatient option. You're at the program roughly 20 or more hours a week, often nearly every weekday, but you sleep at home. PHP fits when symptoms are heavier or you've recently stepped down from inpatient care and aren't quite ready for IOP.
- Residential or inpatient
- You live at the facility for a stretch — often two to four weeks or longer. It's the right call when withdrawal is medically dangerous, when home isn't safe, or when previous outpatient attempts haven't held.
The picture to hold in your head: these aren't a hierarchy where higher equals better. They're a continuum, and the best fit depends on what your life and your body actually need right now.
Why IOP deserves a serious look
If a part of you is thinking, "But isn't real treatment the kind where you go away for a month?" — that's worth pausing on. It's one of the most persistent assumptions about recovery, and the research tells a different story.
A peer-reviewed review of substance use intensive outpatient programs looked at how IOP outcomes stack up against inpatient and residential care. The conclusion was direct: for most individuals, intensive outpatient programs are as effective as inpatient treatment for reducing alcohol and drug use 7. People got similar results — while continuing to live at home, keep their jobs, and stay connected to their families.
That matters for a few reasons. If you've been quietly disqualifying yourself from treatment because you can't take a month off work, you don't have to. If you've been telling yourself outpatient is the "lesser" option, the evidence doesn't back that up for most people. And if a family member is pressuring you toward residential because they assume it's stronger medicine, you now have something concrete to share.
There are real situations where inpatient is still the right first step — dangerous withdrawal, unsafe home environments, severe co-occurring conditions, or repeated outpatient attempts that haven't held. But for a working adult in Southern Maine whose drinking has gotten serious but whose life is still mostly intact, a solid IOP — especially one that includes trauma-informed therapy, medication support, and care for co-occurring mental health — can do the heavy clinical lifting without dismantling the rest of your life 7.
That's not a consolation prize. That's a clinical match.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
How to vet a local program before you commit
Check licensing and credentials in Maine
Before you fall in love with a program's website, check that it's actually licensed to operate. In Maine, that's not a vague endorsement — it's a specific regulatory function. The Maine Department of Health and Human Services, through its Division of Licensing and Certification, runs the Behavioral Health Program that licenses mental health and substance use disorder facilities under state statute 10. Outpatient and intensive outpatient programs have to meet those standards to legally provide care.
What that means for you, on a Tuesday night with a tab open: it's fair to ask a program directly, "Are you licensed by Maine DHHS as a substance use disorder treatment provider?" A legitimate program will answer that without flinching and can point you to documentation. You can also cross-reference with the Maine Office of Behavioral Health, which is the state's central hub for substance use disorder treatment and recovery support information 8.
Beyond the facility license, ask about the people. Who is the medical director, and are they a licensed physician? Are therapists licensed in Maine — LCSWs, LCPCs, LADCs? Is there a clinical director overseeing the program? You don't need to interrogate anyone. You just need real names and real credentials.
Confirm the therapies are evidence-based
This is where a lot of programs blur together on paper. Every website talks about "compassionate, personalized care." Fewer get specific about what actually happens in the room. Your job is to ask.
NIAAA's clinician guidance is clear that effective alcohol use disorder care relies on two pillars: behavioral health treatments and FDA-approved medications, which have been shown to be about equally effective and often work best in combination 5. The behavioral side has names you can listen for. Cognitive behavioral therapy (CBT) helps you spot the thoughts and situations that drive drinking and build new responses. Dialectical behavior therapy (DBT) adds skills for managing intense emotions without reaching for a drink. Motivational interviewing meets you where you are when you're not 100% sure you want to quit. Relapse prevention therapy teaches you to see slips coming before they arrive.
A trauma-informed approach matters too, especially if your drinking is tangled up with old wounds. Trauma-informed simply means the program assumes many people have been through hard things and structures care so it doesn't accidentally retraumatize you.
If a program can't tell you which specific therapies they use, or describes their approach only in feelings-words, that's information. Good programs name their methods plainly and can explain why each one is in the mix.
Ask about medication for alcohol use disorder
Here's something a lot of people don't realize: there are FDA-approved medications specifically for alcohol use disorder, and they actually work. The American Psychiatric Association's practice guideline recommends offering evidence-based pharmacological treatment to patients with AUD when clinically indicated, alongside counseling and psychosocial support 9. Despite that, NIAAA notes these medications are underused in everyday practice — there's a real gap between what the guidelines say and what many programs actually offer 5.
The three medications most often discussed are naltrexone, which can reduce cravings and blunt the reward of drinking; acamprosate, which helps your brain rebalance after you stop; and disulfiram, which causes an unpleasant reaction if you drink while taking it 9. Naltrexone comes in a daily pill or a monthly injection. None of these are sedatives. None of them get you high. And none of them mean you're "replacing one drug with another" — that's stigma talking, not science.
When you call a program, ask directly: "Do you offer medication-assisted treatment for alcohol use disorder? Who prescribes it? Is it integrated with my therapy?" The strongest outpatient programs combine medication with counseling so the same team is coordinating both 5. If a program tells you they don't believe in medication or can't connect you with a prescriber, that's a meaningful limitation — not necessarily a dealbreaker, but something to weigh against your own situation.
Look for integrated care if mental health is part of the picture
If you've been drinking partly to quiet anxiety, dull depression, sleep through PTSD symptoms, or get through a grief you never really processed, you're not unusual. You're describing what clinicians call a co-occurring condition, and how a program handles it matters more than almost any other factor.
So ask, plainly: "Do you treat co-occurring mental health conditions in the same program? Can my therapist here also help me work on the depression and trauma, or will I need a separate provider?" A program built for dual diagnosis can answer that with specifics — which clinicians on staff handle what, how psychiatric medication is coordinated, how trauma is addressed inside the treatment plan. If the answer is essentially "we focus on the drinking and you'd handle the rest somewhere else," you'll want to factor that in.
The intake call: questions worth asking out loud
The first phone call is the part most people dread. You're not expected to have a script. The admissions person on the other end has heard every version of "I don't really know where to start" — that's literally their job. But having a few real questions ready can turn a nervous call into useful information, and you have every right to ask them. Shared decision-making research in substance use care is clear that people who actively participate in choosing their treatment tend to do better, and most patients want exactly that kind of involvement 2.
Keep this short list near you when you call:
- "Are you licensed by Maine DHHS as a substance use disorder treatment program?" 10
- "What level of care do you think fits someone in my situation — standard outpatient, IOP, or PHP — and how do you decide?"
- "Which specific therapies do you use? Do you offer CBT, DBT, motivational interviewing, and trauma-informed care?"
- "Do you prescribe or coordinate medication for alcohol use disorder, like naltrexone or acamprosate?" 9
- "If I also have depression, anxiety, or trauma, will the same team treat that alongside the drinking?" 3
- "What does a typical week look like — how many hours, which days, morning or evening options?"
- "Do you take my insurance, and what would I owe out of pocket?"
- "How soon could I start, and what does the first session look like?"
You don't have to ask all of them. Even three or four will tell you a lot about how a program operates and whether it respects you as a partner in your own care. If the person on the phone gets defensive about plain questions, that's data. If they answer clearly, name their clinicians, and ask thoughtful questions back about your life and history, that's also data — the good kind.
Making it work with a job, a family, and Southern Maine traffic
One of the quiet reasons people put off treatment is the logistics. You're picturing your boss's face when you ask for a month away, your kid's pickup line, the commute from Scarborough or Saco when traffic on I-295 is already a problem at 4:45. Those concerns are real, and a good outpatient program is built around them — not in spite of them.
Strong intensive outpatient programs in the South Portland area typically offer morning, afternoon, and evening tracks specifically so people can keep working. That might mean group from 6 to 9 p.m. three nights a week, or a morning track before your shift starts. You sleep in your own bed. You drive your own kids to school. You eat dinner with your family on the nights you're not in session. The clinical work is intense — group therapy, individual sessions, skill-building, medication coordination when it's part of your plan — but it's stitched into your week instead of replacing it 4.
A few practical things to ask about when you call: Is there an evening track? How flexible is the schedule if a work meeting runs late? Do you offer telehealth for any sessions when weather or a sick kid makes the drive impossible? Can you coordinate with my primary care doctor or psychiatrist? You're allowed to bring your real life into the conversation 2.
Cost, insurance, and what to ask before the first session
Money is the part of this nobody wants to talk about, and the part that stops a lot of people from making the call. So let's be straight about it: most outpatient and intensive outpatient programs in Maine accept commercial insurance and MaineCare, but coverage details vary a lot from plan to plan. You won't know what you actually owe until someone runs your benefits — and any decent program does that for free, before you start.
When you call, ask: "Do you accept my insurance, and can you verify my benefits before my first appointment?" Then ask the follow-ups that matter — what's my copay per session, is there a deductible I haven't met, how many sessions are covered, and do I need prior authorization? If you don't have insurance, ask whether the program offers a sliding scale, payment plans, or can help you apply for coverage through MaineCare or the Maine Office of Behavioral Health, which is the state's central hub for substance use services 8.
You're allowed to ask about money out loud. It doesn't make you less serious about recovery — it makes you a person planning realistically for it.
Your next concrete step
You don't have to solve recovery tonight. You just have to do the next small thing. Pick one program in the South Portland area, look up whether it's licensed by Maine DHHS, and put their number in your phone 10. That's the step. Tomorrow, or whenever you have a quiet ten minutes, call and ask two or three of the questions from earlier — about level of care, evidence-based therapy, and whether the same team treats co-occurring mental health 3. You're allowed to call more than one place. You're allowed to change your mind. If you want a starting point that offers trauma-informed IOP, integrated dual diagnosis care, medication support, and evening tracks built for working adults, Coastal Recovery Partners in South Portland is one option worth that first call. The hardest part was opening the search. You already did it.
Frequently Asked Questions
Do I have to go to inpatient rehab, or can I get real treatment while living at home?
You don't have to go inpatient to get real, clinical treatment. A peer-reviewed review of intensive outpatient programs found that for most individuals, IOPs are as effective as inpatient care for reducing alcohol and drug use 7. Inpatient is the right call when withdrawal is medically risky, home isn't safe, or past outpatient attempts haven't held. For many working adults, IOP does the clinical work without uprooting your life.
How do I know if a local alcohol treatment program is actually licensed and legitimate?
In Maine, substance use disorder programs are licensed by the DHHS Division of Licensing and Certification through its Behavioral Health Program, under specific state statutes 10. Ask any program directly whether they're licensed by Maine DHHS — a legitimate provider will answer plainly. You can also start at the Maine Office of Behavioral Health, the state's central hub for substance use services 8.
What's the difference between outpatient, IOP, and PHP?
They're three points on the same continuum, defined mostly by clinical hours per week 4. Standard outpatient is usually one to two hours weekly — therapy to keep building on progress. Intensive outpatient (IOP) runs about 9 to 20 hours across several days, often with morning or evening tracks. Partial hospitalization (PHP) is roughly 20+ hours weekly, near-daily structure, but you sleep at home. Higher doesn't mean better — it means more support.
Should I ask about medication for alcohol use disorder, or is that only for severe cases?
Ask. The American Psychiatric Association practice guideline recommends offering evidence-based medications — naltrexone, acamprosate, or disulfiram — to patients with alcohol use disorder when clinically indicated, alongside counseling 9. These aren't last-resort tools, and they aren't sedatives. NIAAA notes they're underused in everyday practice, so a program that prescribes or coordinates them is offering something many don't 5. It's a fair question on any intake call.
What if I'm also dealing with anxiety, depression, or trauma alongside drinking?
That's incredibly common, and how a program handles it matters. Research on integrated care for co-occurring mental health conditions shows that treating both together — same team, one coordinated plan — is associated with better engagement and better outcomes than handling them separately 3. Ask whether the program treats dual diagnosis in-house and uses trauma-informed care. The old "get sober first, deal with the rest later" model tends to leave people stuck.
How do I keep my job and family obligations going while in treatment?
That's exactly what outpatient and intensive outpatient programs are built for 4. Strong programs in the South Portland area offer morning, afternoon, and evening tracks so you can keep working, parenting, and sleeping at home. Ask about evening groups, telehealth options for tough weather days, and whether they'll coordinate with your primary care doctor. You're allowed to bring your real schedule into the conversation — good programs expect it 2.
References
- Treatment for Alcohol Problems: Finding and Getting Help. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
- Patient Preferences and Shared Decision Making in the Treatment of Substance Use Disorders: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC4701396/
- Integrating Treatment for Co-Occurring Mental Health Conditions. https://pmc.ncbi.nlm.nih.gov/articles/PMC6799972/
- Chapter 5—Specialized Substance Abuse Treatment Programs. https://www.ncbi.nlm.nih.gov/books/NBK64815/
- Recommend Evidence-Based Treatment: Know the Options. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/recommend-evidence-based-treatment-know-options
- Patient Placement Criteria: Linking Typologies to Managed Care. https://pmc.ncbi.nlm.nih.gov/articles/PMC6876533/
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Substance Use Disorder Services - Maine.gov. https://www.maine.gov/dhhs/obh/support-services/substance-use-disorder-services
- The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. https://pubmed.ncbi.nlm.nih.gov/29301420/
- Behavioral Health - Division of Licensing and Certification - Maine.gov. https://www.maine.gov/dhhs/dlc/licensing-certification/behavioral-health



