
Understanding Substance Abuse Treatment Services

Key Takeaways
- Outpatient care sorts into three levels by weekly hours: standard OP under 9, IOP at 9–19, and PHP at 20+, letting you match intensity to real life without a residential stay.
- A clinical assessment — not self-diagnosis at midnight — determines the right level of care, factoring in withdrawal risk, home stability, co-occurring conditions, and past treatment history.
- Effective programs combine evidence-based therapies like CBT, motivational interviewing, and DBT with medication when appropriate, and treat co-occurring anxiety, depression, or PTSD in the same integrated plan 6.
- Aftercare determines whether early gains hold; one PHP study found 66.7% of alcohol patients abstinent at one month, driven by continued therapy and community meetings 4.
If You're Reading This at 11pm, Start Here
If it's late and you're up looking this up on your phone, that already counts for something. You noticed. You're here.
Maybe you're the one drinking a little more than you meant to again. Maybe it's your partner, your grown kid, your best friend from high school. Either way, you probably picture "treatment" as a 30-day residential stay somewhere far away, and you're quietly ruling yourself out because of your job, your kids, your dog, your rent, or all of the above.
Here's what you may not know yet: substance abuse treatment isn't one door. It's a range of outpatient options that meet you where your week actually is. Some people come in three mornings a week. Some come five. Some do most of it before their workday starts. The point of this guide is to walk you through what those options are, what happens inside them, and how to figure out an honest starting point — without signing your life away.
You don't have to decide anything tonight. Just keep reading.
The Outpatient Ladder: OP, IOP, and PHP Without the Jargon
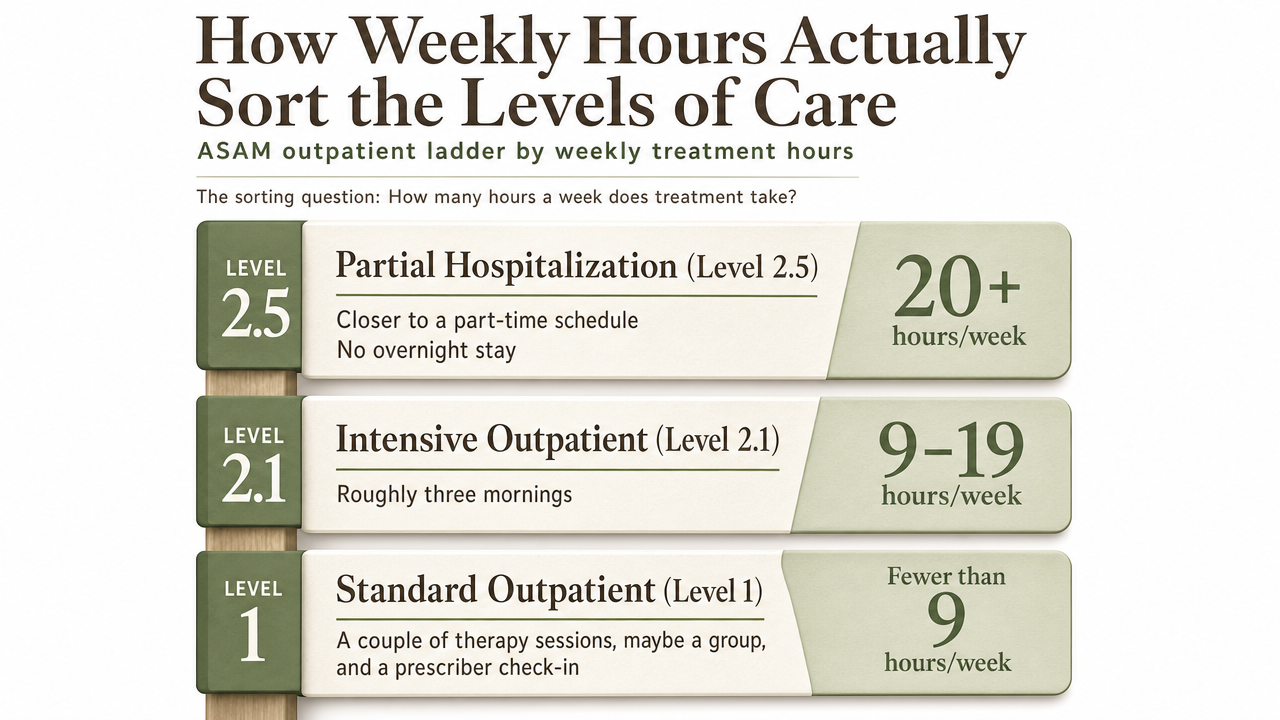
How Weekly Hours Actually Sort the Levels of Care
The alphabet soup — OP, IOP, PHP — is really just a way of asking one question: how many hours a week does your treatment take?
That's it. That's the sorting mechanism.
The American Society of Addiction Medicine (ASAM), which is the ruler most programs measure themselves against, breaks the outpatient world into three main rungs.
- Standard outpatient care, sometimes called Level 1, usually means fewer than 9 hours of clinical time a week. Think of it as a couple of therapy sessions, maybe a group, and a check-in with a prescriber.
- Intensive Outpatient (Level 2.1) sits in the 9–19 hours per week range.
- Partial Hospitalization (Level 2.5) is 20 or more hours per week, without an overnight stay 5.
Read those numbers again with your own calendar in mind. Nine hours a week is roughly three mornings. Twenty-plus hours is closer to a part-time job — you're doing treatment most of the day, several days a week, and going home to sleep in your own bed.
Nobody hands you a menu and asks you to pick. A clinician does an assessment and matches the level of care to what's actually going on: how heavy the use is, whether you've been through a withdrawal that scared you, whether depression or anxiety is stacked on top, and what your home life can absorb.
The point of showing you the hours is simpler. It's proof that "treatment" isn't a single, month-long thing you disappear into. It's a dial that can be turned up or down. Some people start at PHP for a few weeks to stabilize, step down to IOP for structure, and then move to standard outpatient care once the wheels are back on. Others begin at IOP and never need more. A few do well at weekly outpatient from the start.
You're not choosing rehab or nothing. You're choosing an intensity.
What Maine Actually Requires an IOP to Deliver
If you live in the Greater Portland area, there's a floor written into state rules that's worth knowing about. It protects you.
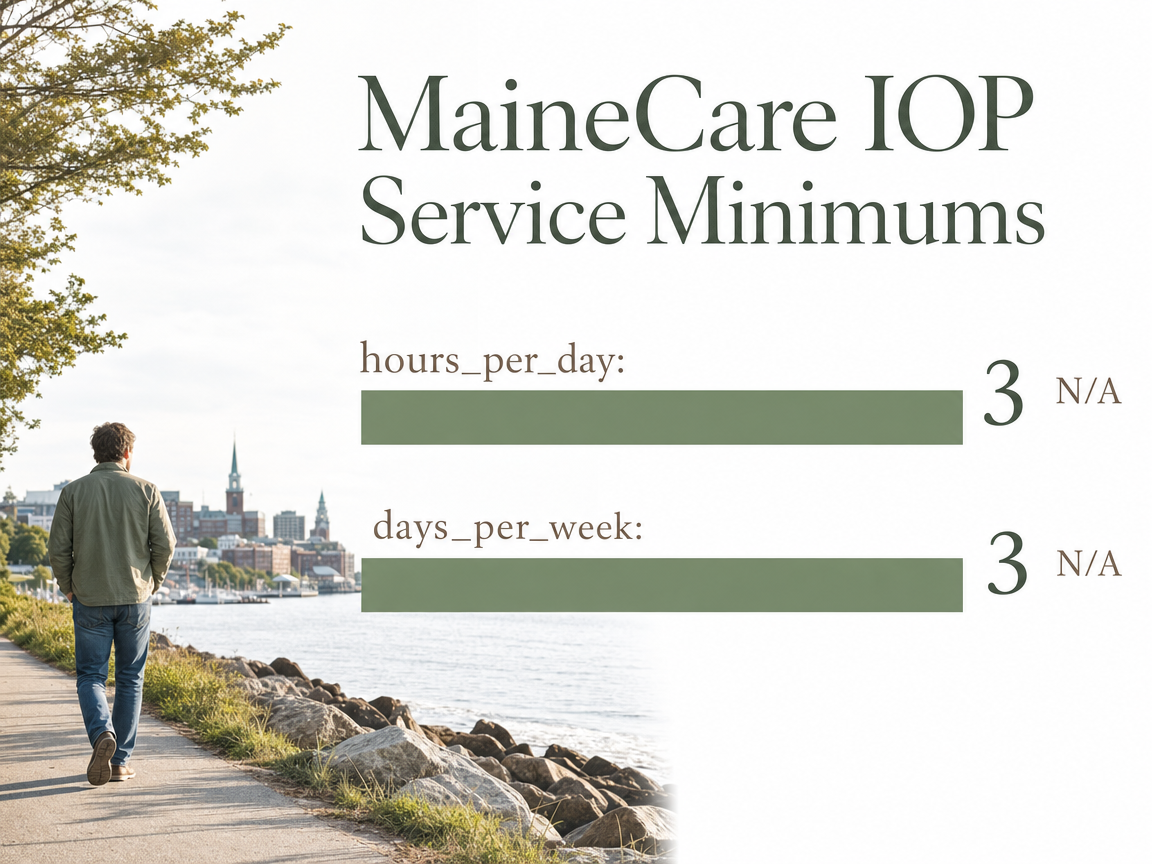
Under MaineCare's behavioral health rules, an Intensive Outpatient Program has to deliver at least 3 hours per day, 3 days per week of qualified services — a short-term, time-limited, multidisciplinary approach, not a loose weekly group 11. Maine's broader substance use disorder regulations echo the same standard: IOPs must be structured, multi-hour clinical and educational programming scheduled at least three days a week, without overnight stays 3.
So when a program in South Portland tells you it runs an IOP, you can hold that description up against something concrete. Are the sessions actually three hours? Do they meet at least three days a week? Is there a real assessment on the front end, counseling, education, and coordination with a prescriber if you need medication?
You're allowed to ask.
You're also allowed to ask what the schedule blocks look like — morning tracks that end before 9am, afternoon groups, evening options after work. The rules set the minimum. The good programs build the schedule around adults who still have to show up for a job, a kid at pickup, or a shift at the hospital.
Do I Really Need Residential Rehab?
Here's the question nobody wants to ask out loud: am I "bad enough" for real rehab, or am I making a mountain out of a molehill?
Both framings are traps. The honest answer isn't about severity theater. It's about safety and structure.
Residential treatment — the 28- or 30-day stay you're picturing — makes sense when:
- Someone can't stay safe at home
- Withdrawal will be medically dangerous
- The living environment itself is fueling the use
- Previous outpatient attempts haven't held
Those are real situations. If any of them describe you, an assessment will say so, and a good clinician will tell you plainly.
But for a lot of adults, that isn't the picture. And the research has caught up to that reality. A comparative effectiveness study found that intensive outpatient programs achieved abstinence and functioning outcomes comparable to inpatient care for appropriately matched patients 15. "Appropriately matched" is doing real work in that sentence — this isn't a claim that IOP replaces residential across the board. It's a claim that for the right person, structured outpatient care isn't a lesser choice. It's a legitimate one.
The practical translation: if you can sleep safely in your own bed, if your withdrawal risk can be managed medically, and if you have some baseline support at home, an outpatient level of care is on the table. You keep your job. You stay in your kid's routine. You still do the work.
The way to find out which lane fits is not to argue with yourself at 11pm. It's to get an assessment and let a clinician help you sort it.
Your First Two Weeks, Step by Step
The Intake Call and the Clinical Assessment
The first call is shorter than you think. Someone picks up, asks what's going on, and listens. You don't need a speech ready. "I'm drinking more than I want to" is enough. "My son has been using and I don't know what to do" is enough.
From that call, you'll get scheduled for a clinical assessment, usually within a few days. Plan on 60 to 90 minutes. A licensed clinician will walk you through your substance use history, your physical health, your mental health, your living situation, your work, your support system, and any past treatment. They'll ask about withdrawal symptoms and safety. Some of the questions will feel personal. That's the point — Maine's outpatient rules specifically require a comprehensive assessment before any level of care is recommended 3.
You are not being graded. You're being matched. The more honest you are, the more useful the recommendation will be. If you've been minimizing for years, this is the first place you get to stop.
How a Level of Care Gets Recommended for You
After the assessment, the clinician pulls it all together and tells you what they're seeing. This isn't a sales pitch for the most intensive program on the shelf. NIDA's foundational principle is that effective treatment attends to multiple needs of the individual, not just drug use — sleep, work, relationships, mental health, medical issues, all of it 1.
You'll usually hear a recommendation shaped like this: a level of care (OP, IOP, or PHP), a therapy schedule, whether medication should be part of the plan, and what an aftercare arc might look like down the road. For co-occurring anxiety, depression, or trauma, integrated, staged care — engagement, stabilization, active treatment, and continuing care — is the standard, not an upsell 6.
You get to ask questions. You get to push back. If a recommendation doesn't fit your life, say so out loud. The plan is a starting point, not a verdict.
The Schedule: Mornings, Evenings, and Real Life
Here's where the abstract becomes your Tuesday.
Once you accept a level of care, you'll be placed into a schedule block. IOP tracks in the South Portland area typically run in the morning (often 9am–noon), afternoon, or evening, three days a week. PHP fills more of the day. Standard outpatient is usually one or two appointments a week that you slot around work.
You'll get a written schedule with group times, individual therapy, and any medication appointments. If you drive a school bus at 6am, tell them. If you can only do evenings because of childcare, tell them. Programs built for working adults expect this conversation.
The first week will feel awkward. New room, new faces, new vocabulary. By week two, most people report the schedule starts to feel like a rhythm rather than an intrusion — which is exactly what it's designed to become.
Inside the Therapy Room: What the Modalities Actually Do
CBT and Motivational Interviewing, in Plain Words
Two names come up over and over: CBT and motivational interviewing. Here's what they actually do once the door closes.
Cognitive Behavioral Therapy (CBT) is the workhorse. You and a counselor slow down a specific moment — the Thursday night you poured a drink after a fight with your spouse, the Sunday you called your dealer instead of going to your niece's birthday — and pull it apart. What was the trigger? What thought showed up? What did the use do for you in that moment? What could go in that slot instead? Across the research on substance use disorders, CBT is one of the most widely studied and effective psychosocial treatments 13, and outpatient CBT-based programs can produce abstinence outcomes comparable to more intensive care for a lot of adults with alcohol problems 12.
Motivational interviewing is the quieter one. Instead of arguing you into change, the counselor asks questions that let you hear your own reasons out loud. Why do you want to cut back? What would be different at home? What's the part of you that still isn't sure? It works because ambivalence isn't a character flaw — it's the honest starting point 13.
DBT Skills for Emotion Regulation and Trauma Histories
Dialectical Behavior Therapy (DBT) shows up in outpatient programs for a reason. If your use tends to spike when emotions get too big — panic, rage, shutdown, that free-fall feeling at 3am — you're not weak. You're missing skills nobody ever taught you.
DBT groups drill four of them:
- Mindfulness
- Distress tolerance
- Emotion regulation
- Interpersonal effectiveness
Concrete practices, not vibes. Ice on the wrists when a craving spikes. A paced breath before a hard conversation. A script for saying no to your brother-in-law's beer. A systematic review of DBT-adapted interventions for substance use found meaningful reductions in substance use, especially for people carrying trauma histories or intense emotion regulation struggles 14.
Why Trauma-Informed Care Is a Baseline, Not a Perk
You'll see "trauma-informed" on a lot of program websites. Ask what it actually changes.
In practice, it means the clinicians assume that a meaningful portion of the people walking in are carrying old wounds — abuse, loss, medical trauma, combat, a childhood you don't want to talk about yet — and they design the room around that. You're not pressured to disclose before you're ready. Group facilitators watch for what re-traumatizes people (surprise confrontation, forced sharing, harsh consequences) and don't do it. Safety, choice, and collaboration are treated as clinical requirements, not soft skills.
SAMHSA's guiding principles for people with co-occurring conditions point in the same direction: integrated, staged care that moves through engagement, stabilization, active treatment, and continuing care — with the therapeutic relationship treated as the foundation the rest of the work sits on 6. If a program can't tell you specifically how it does this, keep looking.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Medication as Part of Treatment, Not a Shortcut Around It
Some people hear "medication-assisted treatment" and picture trading one drug for another. That's not what's happening.
For opioid use disorder, three medications do most of the work: methadone, buprenorphine, and naltrexone. A 2023 review calls methadone the current gold standard, while buprenorphine sits close behind — highly effective, with a lower overdose risk profile, and available in office-based settings rather than only at a dedicated opioid treatment program 7. Naltrexone works differently, blocking the effects rather than easing the craving, and fits some people better than others. For alcohol use disorder, medications like naltrexone and acamprosate can quiet the pull enough to let therapy actually land.
In Maine, this isn't a fringe conversation. MaineCare's opioid health home rules build medication into the level of care itself, requiring counseling hours alongside medication at induction and intensive outpatient levels — the medication and the therapy are supposed to move together, not in separate lanes 10.
When Anxiety, Depression, or PTSD Are Riding Alongside
If drinking or using is only half of what's going on, you already know it.
The panic attacks that started before the wine did. The depression that made the pills feel like a solution. The nightmares that never went away after the accident, the deployment, the childhood you don't talk about. When a mental health condition sits underneath the substance use, treating just one side leaves the other side to pull you back.
Clinicians call this co-occurring disorders, and the standard of care isn't to send you to two different places that don't talk to each other. SAMHSA's guidance is clear: the substance use and the mental health condition should be treated together, in the same program, by a team that shares notes — with care that moves through engagement, stabilization, active treatment, and continuing care as one arc, not two 6.
What that looks like on a Tuesday: your therapist knows about the PTSD when they're helping you plan around a craving. Your prescriber knows about the drinking when they're adjusting an antidepressant. Group topics include emotion regulation and grief, not just relapse triggers.
When you tour a program, ask directly: how do you treat both at once, and who on the team handles the mental health side? A vague answer is an answer.
Telehealth, Scheduling, and Working Around a Real Life
The reason a lot of people never start treatment isn't willingness. It's logistics.
You can't miss the 7am shift. You're the only pickup at 3pm. Your job travels. The nearest program is 40 minutes each way and you'd have to explain the truck in the parking lot every Tuesday. These are real barriers, and they used to end the conversation.
They don't have to now. Telehealth for substance use treatment expanded substantially during the pandemic — outpatient counseling, IOP groups, and medication management delivered by video — and the research that came out of that period shows many patients successfully engaged in remote intensive services, with expanded telehealth meaningfully increasing access to care 16. Some programs now run hybrid tracks: a couple of days in person, a couple over video, with individual therapy scheduled around your work.
Ask three questions when you call:
- Do you offer video groups?
- What time blocks are available — early morning, evening, weekend?
- Can the schedule flex if my shift changes?
A program built for working adults will have answers, not apologies.
Aftercare Is Structural, Not Optional
The program you leave matters as much as the program you enter.
That sounds like a slogan until you look at what the numbers do after discharge. In a study of alcohol treatment patients leaving a partial hospitalization program, about 66.7% were abstinent at the one-month mark — and the patients who stayed abstinent were the ones who kept seeing a mental health provider and kept showing up to 12-step meetings after they walked out the door 4. That's a specific scope: alcohol treatment patients, one month post-discharge from a PHP. Read it that way. But the direction it points is hard to miss.
Two-thirds is a real number. It's also a number that could go up or down depending on what happens in week two, week six, week twelve. Aftercare is the reason it holds.
Good aftercare isn't a pamphlet handed to you on your last day. It's built into the plan from the beginning: a step-down from PHP to IOP to standard outpatient, a standing appointment with a therapist you already know, a prescriber who keeps managing your medication, a group that meets in the community, a check-in call at 30 days. When you're touring a program, ask what discharge actually looks like. Ask who calls you next month. Ask how the handoff works if you move from IOP to a weekly session. If nobody can answer, that's information.
You're not planning for failure by planning for aftercare. You're doing the thing that makes the first program worth the hours you put in.
Picking a Starting Point Without Overcommitting
You don't have to know which level of care you need. You just have to make one call.
An assessment is not a contract. It's a conversation with someone who does this every day, followed by a recommendation you can accept, modify, or sleep on. If a program pushes you into a schedule before anyone has taken a real history, that tells you something. If a program asks about your work, your kids, your mental health, your past attempts, and what you can actually sustain in a week — that tells you something too.
A few practical moves for the week ahead:
- Call one outpatient program in the South Portland area and ask for an assessment.
- Have your insurance card nearby; ask about verification and care coordination up front.
- Write down the three things that scare you most about starting, and bring the list.
- If a friend or partner can sit in the waiting room, let them.
You're not committing to a year of your life. You're committing to one honest conversation. That's the whole first step.
Frequently Asked Questions
Will my insurance cover outpatient substance abuse treatment?
Most commercial plans and MaineCare cover outpatient, IOP, and PHP services when a clinical assessment supports the level of care. Coverage details — copays, session limits, prior authorization — vary. When you call a program, ask them to verify your benefits before your first appointment and to walk you through what your out-of-pocket share looks like. That's a normal request.
Can I do treatment over telehealth, or do I have to show up in person?
Both are options at many programs now. Telehealth for substance use treatment expanded significantly during the pandemic, and research shows many patients successfully engaged in remote counseling, IOP groups, and medication management over video 16. Some programs run hybrid tracks — a couple of days in the building, the rest by video. Ask what the mix looks like and whether the schedule flexes.
Do I have to tell my employer I'm going to treatment?
No, not usually. Your medical records are protected, and many people schedule around work using morning or evening tracks without disclosing anything. If you need job-protected time off, the Family and Medical Leave Act may apply, and human resources only needs to know you have a health condition requiring treatment — not the diagnosis. A care coordinator at the program can help you think this through.
Can my partner or family be involved in my treatment?
Yes, and it often helps. Most outpatient programs offer family sessions, education nights, or coaching for the people who live with you — with your written permission. You get to decide what's shared and when. If someone close to you wants to sit in on an intake call or a family group later, tell the program up front so they can build it in.
What if I'm not sure I have a 'bad enough' problem to need treatment?
Then an assessment is exactly the right call. You don't need to hit a bottom to qualify. If your drinking or using is costing you sleep, relationships, focus, or peace of mind, that's enough of a reason to talk to someone. A clinician might recommend a couple of standard outpatient sessions rather than an intensive program. You'll leave with information, not a verdict.
How long does outpatient treatment usually last?
It depends on the level and how you respond. IOP often runs 8 to 12 weeks, then steps down to less intensive care. PHP is typically shorter and more front-loaded. Standard outpatient can continue for months as maintenance. NIDA's guidance is that treatment should last long enough to produce stable change — not a fixed number of days, but what your recovery actually needs 1.
References
- Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- Principles of Drug Abuse Treatment for Criminal Justice Populations: A Research-Based Guide. https://nida.nih.gov/sites/default/files/podat_cj_guide_508.pdf
- 10-144 C.M.R. ch. 123, § 23 - Substance Use Disorder Services. https://www.law.cornell.edu/regulations/maine/10-144-C-M-R-ch-123-SS-23
- Alcohol Treatment Outcomes Following Discharge From a Partial Hospital Program. https://pmc.ncbi.nlm.nih.gov/articles/PMC6419972/
- 2.1: Intensive Outpatient Services & 2.5: Partial Hospitalization (ASAM Level 2.0 Overview). https://www.pa.gov/content/dam/copapwp-pagov/en/ddap/documents/professionals/documents/asam-page/asam-archive/level%202.0%20iop%20php%20slides.pdf_august2021.pdf
- Chapter 2—Guiding Principles for Working With People Who Have Co-Occurring Disorders. https://www.ncbi.nlm.nih.gov/books/NBK571016/
- A Comparison of Medication-Assisted Treatment Options for Opioid Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC11805484/
- Recently Adopted Rules – Maine Department of Health and Human Services, Office of MaineCare Services. https://www.maine.gov/dhhs/oms/about-us/policies-rules/recently-adopted-rules
- Effect of an Intensive Outpatient Program to Augment Primary Care for High-Need Veterans Affairs Patients: A Randomized Clinical Trial. https://pubmed.ncbi.nlm.nih.gov/28027338/
- MaineCare Benefits Manual, Chapter II, Section 93 – Opioid Health Home Services (Draft/Rule Text). https://www.maine.gov/sos/sites/maine.gov.sos/files/content/assets/c2s093.docx
- MaineCare Benefits Manual, Chapter II, Section 65 – Behavioral Health Services. https://www1.maine.gov/sos/sites/maine.gov.sos/files/content/assets/c2s065.docx
- Outpatient Treatment of Alcohol Use Disorders: A Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC4436276/
- Evidence-Based Practices for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC5715025/
- Dialectical Behavior Therapy for Substance Use Disorders: Systematic Review. https://pubmed.ncbi.nlm.nih.gov/30554575/
- Comparative Effectiveness of Intensive Outpatient Programs vs Inpatient Treatment for Substance Use Disorders. https://pubmed.ncbi.nlm.nih.gov/31986096/
- Telehealth for Substance Use Disorder Treatment During the COVID-19 Pandemic. https://pmc.ncbi.nlm.nih.gov/articles/PMC8288175/


