
Breaking the Cycle with Codependency Treatment

Key Takeaways
- Codependency is a learned relational pattern, not a personality flaw or formal diagnosis, and it carries real costs like anxiety, depression, and lower life satisfaction 1.
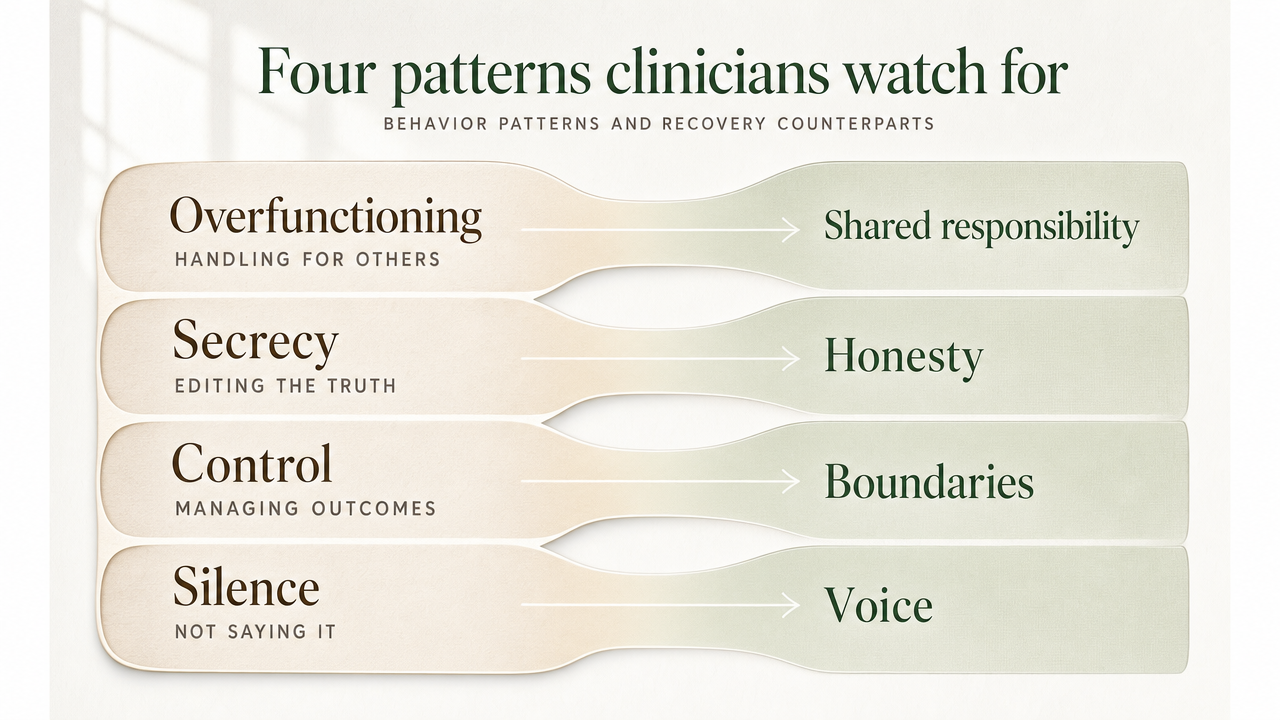
- Clinicians watch for four clustering behaviors — overfunctioning, secrecy, enabling, and self-erasure — each of which has a recovery counterpart you can practice 3.
- Trauma, substance use, and codependent patterns feed each other, so integrated care that treats them together outperforms splitting them across separate providers 5, 7.
- Outpatient levels — standard OP, IOP, and PHP — let you keep working and parenting while doing the real work, so pick the intensity you'll actually attend 6.
When caretaking starts costing you yourself
You know the feeling. The phone buzzes and your stomach drops before you've even looked at the screen. You're already running the math — who needs what, who's upset, what you can fix before it breaks. Somewhere along the way, your own appointments slid off the calendar. Your own feelings got filed under "later."
If you're reading this, you probably already suspect the pattern has a name. You may have called it codependency, or enabling, or just "being the responsible one." What the research actually shows is sobering and, in a strange way, hopeful: these patterns are tied to real mental health costs — anxiety, depression, low self-esteem, and lower life satisfaction 1. They're not just personality quirks. They're not signs you love too much. They're learned responses, often shaped by trauma and by living close to someone else's substance use or mental illness.
That means they can be treated. Not with slogans, and not by leaving your whole life behind. With real, integrated care — the kind that addresses what's happening in your nervous system, your relationships, and your daily routines all at once. That's what the rest of this guide is about.
What codependency actually is — and what it isn't
A learned pattern, not a personality verdict
Here's the part that often surprises people: codependency isn't a diagnosis stamped on your file, and it isn't a flaw stitched into who you are. Researchers describe it as a learned relational pattern — a set of responses you picked up, usually in a home or relationship where someone else's distress, drinking, or mental illness took up most of the oxygen. You learned to read rooms. You learned to anticipate. You learned that keeping the peace was your job.
The integrative review of the codependency literature ties this pattern to real, measurable mental health costs — anxiety, depression, low self-esteem, and reduced life satisfaction 1. This distinction matters because if codependency were a personality verdict, you'd be stuck with it. Because it's learned — shaped by experience, reinforced by environment, often layered on top of trauma — it can be unlearned. Slowly, with help, in small specific moves. The same brain that learned to scan for someone else's mood can learn to check in with your own.
The construct debate clinicians are honest about
You deserve the real picture here. Among clinicians and researchers, there's an ongoing debate about whether codependency is its own distinct condition or whether it overlaps so heavily with things like attachment insecurity and anxiety that it doesn't need a separate label 1. What does that mean for you? It means a good clinician won't hand you the word "codependent" like a permanent ID badge. They'll look at the actual behaviors, the relationships, the trauma history, and the symptoms underneath — and treat those. The label is a shorthand. Your nervous system, your relationships, and your daily life are the real work.
What it looks like in daily life
Four patterns clinicians watch for
Forget the quiz. A good clinician isn't looking for a personality type — they're watching for behaviors, the kind that show up in your calendar, your text threads, and the quiet things you do not say. Family-systems research on substance use disorders points to four patterns that tend to cluster together when someone's life has been organized around another person's drinking, using, or mental health crisis 3. You may recognize all four. You may recognize one.
Overfunctioning. You're handling things that aren't yours to handle — the bills, the apologies to their boss, the explanations to the kids. You tell yourself it's just easier. It is, in the short term. It is also exhausting.
Secrecy. You've started editing the truth about what's happening at home. You minimize to your sister. You change the subject at work. The story you tell the outside world and the story you live inside have drifted apart.
Enabling. You smooth the consequences that might otherwise wake your loved one up — paying the fine, calling in sick on their behalf, replacing the lost phone again. You know it on some level. You also can't quite stop.
Self-erasure. Your own preferences have gone quiet. You can't easily say what you'd want to eat tonight, what you'd do with a free Saturday, what hurts. You've been reading other people's signals for so long that yours have gone dim.
What's useful about naming these patterns is that each one has a recovery-pattern counterpart you can learn — sharing the load instead of carrying it, telling the truth in safe places, letting natural consequences land, and slowly remembering what you actually want. None of that happens at once. It happens in pieces, with support.
How addiction in a partner reshapes you
Living with someone who is actively using changes you. Not because you're weak, and not because you chose it — because your nervous system adapted to a moving target. Research on partners of men with substance use disorders found measurably higher codependency scores in those partners, with personality traits shaping how much the pattern took hold 2. Translation: this is not in your head. The environment did real work on you.
You may notice you've become an expert in someone else's moods and a stranger to your own. You sleep lightly. You scan the driveway. You rehearse conversations before they happen. Over time, family members in these situations often report elevated stress, anxiety, and a quality of life that has narrowed without their permission 10.
Here's what's worth holding onto: the same adaptiveness that made you hypervigilant can be redirected. The skill of reading a room can become the skill of reading yourself. That redirection is exactly what trauma-informed outpatient care is built to do.
Why codependency, trauma, and substance use belong in one treatment plan
The co-occurring picture most articles miss
Most articles about codependency talk to you as if you are standing outside the storm, watching someone else struggle. If that's you, the information still applies. But there's another reader these articles tend to miss — the person who is inside the storm too. The one whose own anxiety, depression, PTSD, or substance use is tangled up with the relationship patterns they came here to read about. If that's closer to your situation, you are not an edge case.
SAMHSA's summary of the 2024 National Survey on Drug Use and Health puts the number at roughly 21.2 million U.S. adults living with both a mental illness and a substance use disorder at the same time 5. That's a lot of people carrying two diagnoses, often quietly, often while still showing up at work and at the dinner table. And many of them are also carrying a third layer — the codependent dynamics that grew up around their mental health symptoms, their substance use, or someone else's.
Here's why that matters for your treatment. Trying to pull those threads apart and treat them in three separate places — one therapist for the depression, one program for the drinking, a self-help book for the relationship patterns — usually doesn't hold. The threads keep tugging each other. Both NIMH and SAMHSA point to integrated care, where mental health treatment and substance use treatment happen in one coordinated setting, as the standard for people with co-occurring conditions 5, 6. Codependent patterns fit naturally into that same plan, because they are shaped by the same trauma history and the same nervous system you're already bringing into the room.
You do not have to get sober first to treat trauma
You may have heard some version of this advice: get sober first, then we'll deal with the trauma. It sounds responsible. It is also, by current clinical guidance, often wrong.
NIDA's work on trauma and addiction helps explain why concurrent care matters so much. Traumatic experiences — abuse, neglect, family conflict, violence — are tightly associated with the development of substance use disorders, and many people with PTSD also live with an SUD 4. The trauma and the substance use are often feeding each other. The codependent patterns wrapped around them are part of the same survival system.
If a provider tells you to white-knuckle through sobriety before they'll look at your trauma history, that is worth questioning. A trauma-informed outpatient program can hold all of it at once, in the right sequence, at a pace your nervous system can actually use.
What evidence-based codependency treatment actually does
CBT for the thoughts that keep you over-responsible
Cognitive behavioral therapy doesn't argue with your love for the person you're worried about. It works on the thoughts that turn that love into a job description. The quiet ones. If I don't fix this, no one will. If I say no, something terrible will happen. Their feelings are my responsibility. Those beliefs feel like facts. CBT slows them down enough for you to see them as predictions — and then test whether the predictions actually come true.
NIMH names CBT among the behavioral therapies with the strongest evidence base for people living with both substance use and other mental health conditions 6. In session, you'll catch a specific thought, examine what it's costing you, and try a small behavioral experiment — declining one request, letting one consequence land — to see what really happens. Usually less than your nervous system predicted.
DBT skills for the feelings underneath the caretaking
Underneath the over-responsibility is usually a feeling you've been outrunning. Panic when someone is angry with you. Guilt that flares the moment you put yourself first. A flatness that sets in after years of swallowing your own needs. Dialectical behavior therapy is built for exactly this terrain — feelings that arrive at full volume and don't respond to reasoning.
DBT teaches concrete skills in four areas: distress tolerance for the moments you'd otherwise rescue someone just to make the discomfort stop, emotion regulation for the slower work of naming and shifting what you feel, interpersonal effectiveness for asking and refusing without collapsing, and mindfulness for noticing your own signals again. None of these are abstract. You practice them in the week between sessions, in real conversations with real stakes. The skill of saying "I need to think about that" instead of an automatic yes is a DBT move. So is sitting through ten minutes of someone else's disappointment without fixing it.
Motivational interviewing when ambivalence is the real obstacle
You may want to change the pattern and dread changing it at the same time. That's not weakness — it's ambivalence, and it's the most common starting point for any real shift. Motivational interviewing is a conversational approach designed for exactly that knot. NIMH lists it alongside CBT as an evidence-supported behavioral therapy for co-occurring conditions 6.
Instead of pushing you toward a decision, a clinician trained in motivational interviewing helps you put both sides of your ambivalence on the table — what you'd lose by changing, what you're already losing by not. The work is collaborative, not corrective. Most people leave those conversations with more clarity than they came in with, and without the defensive crouch that direct advice tends to trigger.
Trauma-focused therapy for the root, not just the pattern
Codependent behaviors are often the visible part of something older. A childhood spent reading a parent's drinking. A relationship where your safety depended on someone else's mood. NIDA describes a strong association between traumatic experiences — abuse, neglect, family conflict, violence — and the development of substance use disorders, with PTSD and SUD frequently traveling together 4. The relational patterns you learned in those environments are part of the same survival system.
Trauma-focused therapies treat the root, not just the behavior on the surface. VA professional guidance supports evidence-based approaches like Prolonged Exposure, Cognitive Processing Therapy, and EMDR for people with co-occurring PTSD and SUD, delivered alongside substance use care rather than after it 7. The goal isn't to relive what happened. It's to help your nervous system file those memories as past instead of present — so the next ask from someone you love doesn't land like an emergency.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Choosing a level of care that fits your real life
You probably can't disappear for thirty days. You have a job, a kid, a parent who needs rides, a dog. The good news is that most evidence-based work for codependent patterns, co-occurring mental health symptoms, and substance use does not require you to vanish. It can be built around your week.
Outpatient care comes in three intensities, and they're meant to step up or down as you do.
Standard outpatient (OP) usually means one to a few hours a week — individual therapy, sometimes a group, often the right level once you've stabilized and you're maintaining gains.
Intensive outpatient (IOP) typically runs around nine to twelve hours a week across multiple days, with a structured mix of group, individual, and skills work. It's enough scaffolding to actually change patterns, and most programs offer morning, afternoon, or evening tracks so you can keep working.
Partial hospitalization (PHP) is the most intensive non-residential option, usually around twenty hours a week, for people who need close clinical contact but can still sleep at home.
If you're carrying co-occurring conditions, ask whether the program treats mental health and substance use in one coordinated plan rather than handing you off 6. For trauma, ask whether you can begin trauma-focused work alongside SUD care, not after it 7. The right level is the one you'll actually attend this week.
Why the gap between needing help and getting it stays wide
Here's a number worth sitting with for a moment. In the 2024 National Survey on Drug Use and Health, only 19.3% of people aged 12 or older who needed substance use treatment in the past year actually received it 8. About one in five. That figure measures SUD treatment engagement specifically — not codependency support, not mental health care — but it tells you something honest about how steep the path to help still is, even when the need is clear.
You probably already know some of the reasons, because you're carrying them. The job that won't pause. The kids who need dinner. The shame of admitting how bad it's gotten. The fear that asking for help will rearrange your life in ways you can't predict. And if your situation involves both mental health symptoms and substance use, the maze gets harder — different providers, different intake forms, different waitlists, each one asking you to tell the story again.
None of that means you're failing. It means the system has been built in ways that punish exactly the people most likely to need it. Recognizing that is part of what makes flexible outpatient care — evening tracks, IOP and PHP options, integrated mental health and SUD treatment in one place — worth asking about by name. You shouldn't have to disappear to get well.
What family members carry — and why their care matters
If you've been the steady one in someone else's storm, your body has been keeping a tally even when you haven't. Research on relatives of people with addiction finds they often live with elevated stress, anxiety, and a quality of life that has quietly narrowed — sleep, hobbies, friendships, all thinned out by years of being on call 10. The cost is real, and it is not imagined.
That's why the people around the person in treatment need care of their own, not as a favor and not as backup. Family-focused work belongs in the same plan as substance use and mental health treatment, because the patterns that grew up in the household — overfunctioning, secrecy, smoothing over consequences — don't just dissolve when one person gets sober 3. They need their own attention. Family sessions, skills groups, and your own individual therapy can run alongside a loved one's outpatient program, or stand on their own if they're the one not yet ready. Your recovery is not contingent on theirs.
A first week of small, specific moves
You don't have to overhaul your life by Sunday. The work of unlearning a codependent pattern happens in small, specific moves, and the first week is mostly about gathering information and lowering the stakes.
Day 1 or 2. Write down three moments this week when your stomach dropped before you read a text. Just notice. No fixing yet.
Midweek. Pick one small request you'd normally auto-yes to and say, "Let me think about that, I'll get back to you tonight." That sentence is a complete skill.
Anytime. Call SAMHSA's free, confidential 24/7 helpline for a referral, or reach out to a local trauma-informed outpatient program directly to ask about IOP, PHP, or standard outpatient options that fit your schedule 9. In South Portland, Coastal Recovery Partners offers that kind of integrated, dual-diagnosis care.
One honest sentence, one paused yes, one phone call. That's the week. Every step forward counts.
Frequently Asked Questions
Is codependency a mental health diagnosis?
No. Codependency is not a formal diagnosis in the DSM. Researchers describe it as a learned relational pattern linked to anxiety, depression, low self-esteem, and reduced life satisfaction, and there's honest debate about whether it overlaps too heavily with attachment insecurity to stand on its own 1. A good clinician treats the underlying symptoms and behaviors, not the label.
Do I have to wait until my loved one gets sober before I start treatment?
No. Your recovery isn't contingent on theirs. Family members living close to active addiction often carry elevated stress, anxiety, and a quality of life that has narrowed without their consent 10. You can begin individual therapy, family-focused work, or a structured outpatient program now, whether or not your loved one is ready. Starting on your own is allowed.
Can I treat codependency, trauma, and substance use at the same time?
Yes, and current guidance supports it. VA professional guidance concludes that patients with co-occurring PTSD and substance use disorder can tolerate and benefit from trauma-focused therapy delivered alongside SUD care, not only after abstinence 7. Integrated outpatient programs are designed to hold mental health, substance use, and the relational patterns wrapped around them in one coordinated plan.
What kind of therapy works best for codependent patterns?
There's no single right answer, but the evidence-based approaches NIMH points to for co-occurring conditions — cognitive behavioral therapy and motivational interviewing — translate well to codependent patterns 6. CBT works on the thoughts that keep you over-responsible. DBT teaches distress tolerance, emotion regulation, and interpersonal skills. Trauma-focused therapy treats the root underneath the behavior. Most plans blend several.
Will I have to leave work or family to get this kind of care?
Usually not. Outpatient care is built around your week. Standard outpatient is a few hours weekly. Intensive outpatient (IOP) typically runs nine to twelve hours across several days, often with morning, afternoon, or evening tracks. Partial hospitalization (PHP) is more intensive but still lets you sleep at home. Many people in South Portland keep working while attending 6.
How do I know if what I'm experiencing is codependency or just caring deeply about someone?
Caring deeply doesn't cost you yourself. Codependent patterns do. Watch for the four behaviors clinicians flag in family-systems research: overfunctioning, secrecy, enabling, and self-erasure 3. If your own preferences have gone quiet, if you're editing the truth, if you can't say no without panic — that's worth bringing to a trauma-informed clinician. Love isn't the problem. The pattern is.
References
- Co-Dependency Revisited: An Integrative Review of the Literature. https://pmc.ncbi.nlm.nih.gov/articles/PMC13067074/
- Living with Addicted Men and Codependency: The Moderating Effect of Personality Traits. https://pmc.ncbi.nlm.nih.gov/articles/PMC5115643/
- The Impact of Substance Use Disorders on Families and Children. https://pmc.ncbi.nlm.nih.gov/articles/PMC3725219/
- Trauma and Stress | National Institute on Drug Abuse (NIDA). https://nida.nih.gov/research-topics/trauma-and-stress
- Co-Occurring Disorders and Other Health Conditions | SAMHSA. https://www.samhsa.gov/substance-use/treatment/co-occurring-disorders
- Finding Help for Co-Occurring Substance Use and Mental Disorders. https://www.nimh.nih.gov/health/topics/substance-use-and-mental-health
- Treatment of Co-Occurring PTSD and Substance Use Disorder in VA. https://www.ptsd.va.gov/professional/treat/cooccurring/tx_sud_va.asp
- SAMHSA Releases Annual National Survey on Drug Use and Health. https://www.samhsa.gov/newsroom/press-announcements/20250728/samhsa-releases-annual-national-survey-on-drug-use-and-health
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- How do psychological characteristics of family members affected by addiction influence their quality of life?. https://pmc.ncbi.nlm.nih.gov/articles/PMC6620238/



