
How to Choose Local Rehab Centers That Fit Your Life

Key Takeaways
- Choose a program based on fit between clinical care, your real schedule, and your finances, because the most photogenic facility still fails if it does not match your life 1.
- Understand what outpatient, IOP, PHP, residential, and inpatient actually mean week to week, then pick the level you can realistically show up for and that matches the severity of what is happening 2.
- Ask programs by name about CBT, DBT, motivational interviewing, and trauma-informed care, and listen for specific answers, since effective treatment combines behavioral therapy with appropriate medical supports 18.
- For opioid use disorder, insist on medications like buprenorphine, methadone, or naltrexone, because detox alone raises the risk of relapse and overdose 7; for alcohol, ask which FDA-approved medications are offered 17.
- Plan around transportation, work hours, family duties, and telehealth options before committing, since these practical barriers are what most often pull people out of treatment early 9.
- Ask plainly about network status, covered levels of care, prior authorization, copays, and sliding-scale options, knowing that parity rules require substance use coverage comparable to medical and surgical care 14.
- Verify licensing through Maine's Division of Licensing and Certification, confirm medication standards, and ask who the medical and clinical directors are before sharing your insurance card or your story 13.
- Treat intake as a two-way conversation by bringing specific questions about scheduling, missed sessions, and step-downs, because shared decision-making improves referral follow-through and ongoing engagement 11.
Start with fit, not features
If you're reading this, you've probably already done the hardest part of the day: you've admitted that something needs to change, and you've opened a browser instead of closing the tab. That counts. Let's make the next hour useful.
Most rehab websites you'll land on tonight will sell you features — a peaceful setting, a chef-prepared menu, a fitness room, a list of therapy acronyms in bold. Features are easy to photograph. They are not what decides whether treatment works for you. The thing that decides that is fit.
By fit, this guide means three honest questions, asked together: Does the clinical care match what's actually going on with you? Does the schedule and setting match the life you have to keep living — your job, your kids, your commute from Greater Portland, your car situation? And does the financial picture, including your insurance, work without quietly setting you up to quit in week three?
That framing is not a marketing idea. It's lifted from how addiction researchers describe effective care: no single treatment is right for everyone, and matching the setting, services, and intensity to your specific situation is what moves outcomes 1. The reverse is also true. A famous program that doesn't fit your life is a program you will leave.
So before you compare local rehab centers on amenities, get clear on what your life can hold. The rest of this article walks you through exactly how.
Match the level of care to the life you actually have
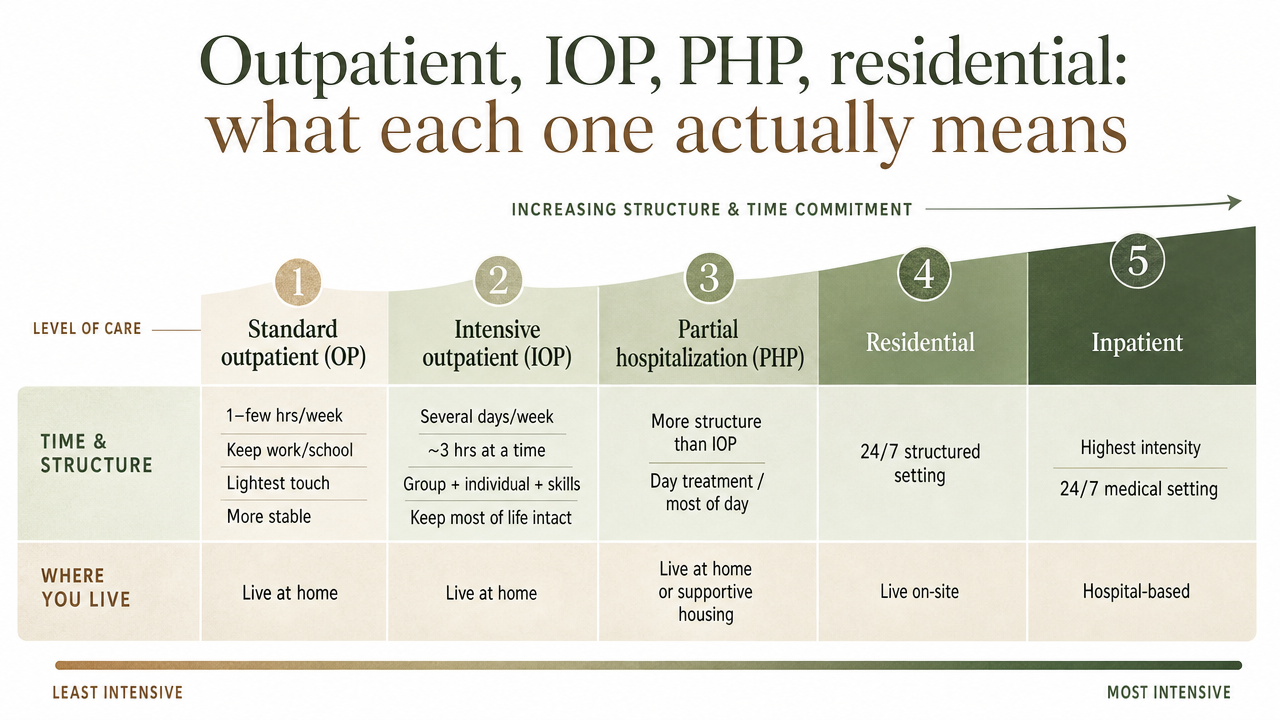
Outpatient, IOP, PHP, residential: what each one actually means
The acronyms get thrown around like everyone already knows them. You don't have to. Here's what each level of care actually looks like in a normal week, in plain language, drawn from how SAMHSA describes the main treatment settings 2.
- Standard outpatient (OP)
- Usually one to a few hours of counseling per week. You live at home. You keep your job. You drive yourself there after work or before the school pickup. It's the lightest touch, and it's a real option when your situation is more stable and you mostly need a steady place to do the work.
- Intensive outpatient (IOP)
- A meaningful step up in structure. Most programs run several days a week, often for three hours at a time, mixing group therapy, individual sessions, and skill-building. You still live at home and still keep most of your life intact. SAMHSA's clinical protocol notes that IOPs offer group, individual, and family services across multiple days per week while patients sleep in their own beds 3.
- Partial hospitalization (PHP)
- The most intensive non-residential level. It's closer to a full-time job in hours — often five or six hours a day, five days a week — but you still go home at night. PHP is what people often step down to after a hospital stay, or step up to when standard outpatient isn't holding.
- Residential treatment
- You live at the facility, typically for weeks. Daily life pauses. Phones, work, and family contact are limited by design.
- Inpatient (hospital-based)
- Short-term medical stabilization, usually for detox or a co-occurring medical or psychiatric crisis.
Read those again with your own week in mind. Which one could you actually show up for on a Tuesday in February? That question matters more than which one sounds the most thorough.
When outpatient is enough, and when it isn't
Here is the part most rehab websites won't tell you straight: outpatient and IOP are not a watered-down version of "real" rehab. A review of intensive outpatient programs concluded that IOPs are viable alternatives to inpatient and residential treatment, with comparable outcomes in substance use reduction when patients are matched to the right level of care 4. Comparable. Not lesser. The catch is the matching.
Outpatient care, including IOP, tends to fit when you can sleep safely at home, when withdrawal isn't medically dangerous, when you have at least one stable person in your corner, and when you can get to sessions without your phone being the only thing standing between you and using again. NIDA's principles point in the same direction: the setting should match the severity of the disorder, any co-occurring mental health conditions, and the realities of your life 1.
It isn't enough — and being honest about this is part of choosing well — when withdrawal needs medical supervision, when your home isn't safe or sober, when you've cycled through outpatient before and need more containment, or when a psychiatric crisis is active alongside the substance use. In those cases, residential or PHP is often the better starting point, not the failure option. Many people start higher and step down to IOP, then to standard outpatient, then to alumni support. That stepped path is the norm, not a detour.
What evidence-based care looks like when you call to ask
Therapies worth asking about by name: CBT, DBT, MI, trauma-informed care
When you call a local rehab center, the person on the phone will say a lot of nice things. Warm. Welcoming. Family. Those words are free. What you're actually trying to find out is whether the clinicians inside the building know what they're doing on a Wednesday afternoon when a group goes sideways. The fastest way to test that is to ask which therapies they use by name, and then listen for whether the answer is specific or vague.
Here are the four to ask about, in plain English.
- CBT — cognitive behavioral therapy
- A structured approach where you and a clinician identify the thoughts and situations that pull you toward using, then build practical skills to interrupt that pattern. It's not a pep talk. It's homework, role-plays, and tracking what actually happens in your week. A review of CBT for substance use disorders found it works both on its own and combined with other treatments, which is why it shows up in almost every serious program 8.
- DBT — dialectical behavior therapy
- A cousin of CBT, with a heavier focus on managing intense emotions, tolerating distress without using, and steadying relationships. If your drinking or using has been tangled up with anxiety, anger, or self-harm thoughts, DBT skills are the ones you want in your pocket.
- MI — motivational interviewing
- Less a therapy and more a conversational style clinicians use to help you talk through your own reasons for change, instead of being lectured into it. You'll know a program uses it when the intake feels like a real conversation, not a sales pitch.
- Trauma-informed care
- Means the program assumes that many people in treatment carry past trauma, and it's built to not re-injure you on the way to recovery — no surprise confrontations, no shaming groups, no clinicians who treat your story as a checkbox.
Federal reviews of evidence-based SUD practice consistently land on the same point: effective care is individualized and combines behavioral therapies with the right medical supports 18. A program that can't explain how it does that, in words you understand, is one to keep questioning.
Medications for alcohol and opioid use disorder
Medication is where a lot of good local programs quietly separate themselves from the rest. If you're dealing with alcohol or opioids, this part matters more than the lobby furniture.
For alcohol use disorder, there are FDA-approved medications that can reduce cravings and the pull to drink. NIAAA frames behavioral treatment, medications, and mutual-support groups as a "full menu" of options that are roughly equally effective and can be combined to fit the person in front of them 17. Translation: if a program tells you medication for alcohol is unnecessary or a crutch, that's a flag. Ask which medications they prescribe, who prescribes them, and how they coordinate that with your therapy.
For opioid use disorder, the stakes are higher and the guidance is sharper. The CDC tells clinicians that medications for opioid use disorder — buprenorphine, methadone, and naltrexone — are associated with reduced risk of overdose and death, and that detoxification alone, without medication, is not recommended because it raises the risk of relapse and overdose 7. Read that twice if you need to. A "detox and willpower" plan for opioids is not equivalent to evidence-based care.
These medications are also regulated. Federal statutes and SAMHSA guidance set specific standards for how opioid use disorder medications can be prescribed and dispensed 6. That's why some local programs offer medication-assisted treatment directly and others refer out — both can be fine, as long as the handoff is real and not a phone number scribbled on a card.
Questions worth asking outright:
- Do you prescribe medication on-site, or coordinate with a prescriber?
- Is medication something I can start during intensive outpatient, or only after?
- How do you decide together when to taper or continue?
An answer that respects your input is the answer you want.
Life fit: schedule, transportation, family, and telehealth
You can find the most clinically sound program in Cumberland County and still drop out by week four if it doesn't fit your week. That's not a character flaw. It's the most common reason people leave treatment early. When researchers asked people seeking or already in substance use treatment what actually got in their way, the answers were not abstract. They named transportation, inconvenient appointment hours, and family responsibilities as the practical barriers that decided whether they could keep showing up 9.
So before you say yes to a program, sit with your real calendar for a minute. Not the ideal version. The one with the 6 a.m. shift, the custody handoff on Wednesdays, the parent you drive to dialysis, the car that's been making that sound. Ask:
Can I get to this building, on these days, at these times, for the next three months? If the program only runs midday groups and you work 9 to 5, the answer is no, no matter how good the clinicians are. Some local outpatient programs run morning, afternoon, and evening tracks specifically so people don't have to choose between treatment and a paycheck. That kind of scheduling flexibility is a clinical feature, not a perk.
What's the transportation plan, honestly? If you're relying on a single car shared with a partner, or on rides from someone whose schedule shifts week to week, your attendance will shift week to week too. Some people solve this with a bus route from downtown Portland; others lean on a sober friend for the first month. Either is fine. No plan is the problem.
Who at home needs to know, and what do they need to do? Family involvement isn't a soft add-on. Reviews of family engagement in substance use treatment find that bringing family in — through education, family therapy, or structured support — meaningfully improves treatment and recovery outcomes 12. Ask whether the program offers family sessions and how often. "We can include them if you want" is a different answer than "family night is the second Tuesday of every month."
And then there's telehealth. If you live a half-hour from the program, or your work travels, or your childcare evaporates twice a month, ask whether sessions can be hybrid. A systematic review of telepsychiatry for addiction treatment found that outcomes for people receiving care by video were similar to outcomes for people receiving in-person care 10. That doesn't mean every session should be on a screen — early treatment often goes better in a room with other humans — but a program that can flex when your week falls apart is a program you're more likely to finish.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Financial fit: insurance, parity, and what to ask before you commit
Money is where good intentions quietly fall apart. You finally pick a program, you start to feel a little hope, and then a billing question you didn't know to ask blindsides you in week two. A few minutes of homework before you sign anything will save you from that.
Start with what the law already gives you. Under federal rules, most health plans have to cover mental health and substance use disorder services, and parity protections require that coverage to be comparable to what the plan offers for medical and surgical care — so things like the number of visits, prior authorization requirements, and out-of-pocket costs for outpatient or IOP shouldn't be quietly worse than they'd be for a physical health condition 14. The specifics depend on your plan and on Maine's marketplace, but the floor is real. You are not asking for a favor.
When you call a local center, ask these out loud, and write the answers down:
- Are you in-network with my insurance?
- Which levels of care — outpatient, IOP, PHP — are covered under my plan?
- What does "medically necessary" mean for getting IOP approved, and who at your office handles that authorization with my insurer?
- What will my copay or coinsurance be per session, and is there a deductible I haven't met?
- If I need medication for alcohol or opioid use disorder, is that billed separately, and through whom?
- If I can't afford the copays, what sliding-scale or payment-plan options exist?
A program that answers those questions plainly — without sighing, without rushing you, without making you feel like the question is rude — is a program that will probably handle the rest of your care the same way. Ask for the answers in writing if it helps. This is not paranoia. This is the kind of attention to your own life that recovery actually rewards.
Is this place legitimate? A short verification checklist
Anyone can put a calming photo of a pine tree on a website. That isn't the same as being a real, regulated clinical program. Before you give a center your insurance card and your story, run through a short check.
- Licensing. In Maine, substance use and mental health programs — including outpatient and intensive outpatient services — are licensed through the state's Division of Licensing and Certification, which sets specific standards programs must meet to operate 13. You can ask a center directly: "Are you licensed by the State of Maine for outpatient and IOP services, and can you share your license?" A legitimate program will not flinch at that question.
- Medication standards. If they offer or coordinate medication for opioid use disorder, they should be able to explain how their prescribing follows federal statutes and clinical guidelines for methadone, buprenorphine, or naltrexone 6. "We just don't believe in medication" is not a clinical answer.
- Named therapies, named clinicians. A real program can tell you which evidence-based therapies it uses, who provides them, and what their credentials are. Effective care combines behavioral therapy with the right medical supports, and reputable centers can show you how they do both 18.
- A clear medical director and clinical lead. Ask who oversees care and who you'd call if something went wrong at 8 p.m. on a Sunday.
If any of those answers come back vague, that's information. Keep dialing.
The intake conversation: how to make it a real dialogue
The first phone call or intake appointment can feel like a job interview where you're not sure what the job is. You want to seem fine enough that they take you seriously, and bad enough that they don't dismiss you. Drop that. The intake is supposed to be a two-way conversation, and you have permission to treat it like one.
Research on shared decision-making in substance use care makes a simple point: when people and clinicians actually talk through the options together, referrals and ongoing engagement go up 11. Translation for you: a good intake clinician will ask what you want, not just tell you what you'll get.
Walk in with a short list. Write it on the back of an envelope if that's what you have.
- What's a typical week here look like for someone at the level you're recommending for me?
- What would you change about the plan if my work schedule shifts?
- If I miss a session because my kid is sick, what happens — clinically and administratively?
- How will you and I decide together when I'm ready to step down, or up, a level?
- If something isn't working in week three, who do I tell, and what changes?
Notice what they do when you ask. A clinician who slows down, answers in plain English, and adjusts the plan based on what you said is showing you how the rest of treatment will feel. One who pushes you into a pre-set track without flinching at your questions is showing you that too. Both are useful information. Pick the program that treats your input as part of the clinical picture, not as an obstacle to it.
Where to start this week if you're in Greater Portland
You don't have to solve the whole thing tonight. You just have to take one small step that moves you off the couch and into a real conversation. Here's what that can look like between now and Friday.
If you're not sure where to begin, call SAMHSA's National Helpline at 1-800-662-HELP. It's free, confidential, open every hour of every day, and a real person will help you sort through local treatment options based on what you tell them 16. You don't need insurance information ready. You don't need to have the right words. They've heard every version of this call.
If you already have a name or two of local programs — places in South Portland, Portland, or somewhere along the commute you actually drive — call them directly. Ask for an intake screening, not a tour. Use the questions from the earlier sections: which levels of care they offer, which therapies by name, how they handle medication for alcohol or opioid use disorder, what your insurance covers, when groups meet. Take notes. Compare two or three places before you decide.
If you're in Greater Portland and looking for a trauma-informed outpatient continuum that runs morning, afternoon, and evening tracks — so treatment can happen around your job and your family — Coastal Recovery Partners is one local example of what that looks like in practice. There are others. The point is that this kind of care exists close to home, and treatment for substance use disorders does work 15. You called. That's the first session.
Frequently Asked Questions
How do I know if I need residential rehab or if outpatient is enough?
Look at safety first, then structure. If withdrawal could be medically dangerous, your home isn't sober, or a psychiatric crisis is active, residential or hospital-based care is the right starting point. If you can sleep safely at home and have some support, outpatient or IOP often fits. The setting should match the severity of your disorder and your real circumstances 1.
What questions should I ask a local rehab center before I commit?
Ask which levels of care they offer, which therapies they use by name, and how they handle medication for alcohol or opioid use disorder. Ask about scheduling, family involvement, insurance, and what happens if you miss a session. A good intake clinician treats this as a shared conversation, not a script, and that collaboration itself improves engagement in care 11.
Will my insurance actually cover rehab in Maine?
Most likely, yes, at least in part. Federal rules require most health plans to cover mental health and substance use services with parity protections, meaning coverage should be comparable to medical and surgical care 14. Specifics depend on your plan. Call the center and ask if they're in-network, which levels of care are covered, what "medically necessary" means for approval, and what your copay will be.
Can I keep working or caring for my kids while in treatment?
That's exactly what outpatient and intensive outpatient care are built for. IOPs typically meet several days a week, often with morning, afternoon, or evening tracks, and you live at home throughout 3. Research on what keeps people in treatment points to schedule, transportation, and family responsibilities as the biggest barriers 9, so a program that flexes around your week is doing clinical work, not a favor.
Is telehealth a real option for addiction treatment, or just a workaround?
It's real. A systematic review of telepsychiatry for people with substance use disorders found that outcomes were similar to in-person care 10. That said, telehealth works best as part of a plan, not the whole plan, especially early on. Hybrid programs that mix in-person groups with video sessions when your week falls apart tend to be the most sustainable for working adults and caregivers.
How can I tell if a local program is legitimate and uses evidence-based care?
In Maine, ask whether the program is licensed by the Division of Licensing and Certification for outpatient and IOP services 13. Then ask which evidence-based therapies they use, how they prescribe or coordinate medication for opioid and alcohol use disorder, and who their medical and clinical directors are. Effective care combines behavioral therapy with appropriate medical support, and real programs can show you both 18.
References
- Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- TIP 47: Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. https://www.samhsa.gov/resource/ebp/tip-47-substance-abuse-clinical-issues-intensive-outpatient-treatment
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- What Types of Alcohol Treatment Are Available?. https://alcoholtreatment.niaaa.nih.gov/what-to-know/types-of-alcohol-treatment
- Substance Use Disorders: Statutes, Regulations, and Guidelines. https://www.samhsa.gov/substance-use/treatment/statutes-regulations-guidelines
- Opioid Use Disorder: Treating. https://www.cdc.gov/overdose-prevention/hcp/clinical-care/opioid-use-disorder-treating.html
- Cognitive-Behavioral Therapy for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC2897895/
- Barriers and Facilitators to Substance Use Disorder Treatment: Perspectives from People Seeking or Using Treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC9434658/
- The Efficacy of Telepsychiatry in Addiction Patients: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC10213379/
- A Shared Decision-Making Tool to Prevent Substance Abuse. https://pmc.ncbi.nlm.nih.gov/articles/PMC5785681/
- Family Involvement in Treatment and Recovery for Substance Use Disorders among Transition Age Youth: Research Bedrock and Opportunities. https://pmc.ncbi.nlm.nih.gov/articles/PMC8380649/
- Behavioral Health - Division of Licensing and Certification (Maine). https://www.maine.gov/dhhs/dlc/licensing-certification/behavioral-health
- Mental health & substance abuse coverage. https://www.healthcare.gov/coverage/mental-health-substance-abuse-coverage/
- Substance Use Disorders Treatment Options. https://www.samhsa.gov/blog/substance-use-disorders-treatment-options
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Recommend Evidence-Based Treatment: Know the Options. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/recommend-evidence-based-treatment-know-options
- Evidence-based practices for substance use disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC3678283/
- Treatment Approaches for Drug Addiction. https://www.drugabuse.gov/publications/drugfacts/treatment-approaches-drug-addiction



