
What to Ask an Outpatient Alcohol Detox Near Me

Key Takeaways
- The intake call is a screening conversation, not a sales pitch — you're checking whether a program can safely manage withdrawal and connect you to ongoing alcohol use disorder care 2.
- Outpatient detox only fits people with mild withdrawal, medical stability, and sober support at home; seizure history, DTs, or unstable conditions require medically managed inpatient care 5.
- Ask ten specific questions covering written protocols, CIWA-Ar scoring, reassessment, medications, scheduling, aftercare, co-occurring conditions, after-hours access, cost, and relapse response to separate serious programs from vague ones 1.
- Strong answers name medications, scales, and on-call clinicians; vague reassurance, pressure to commit, or skipping naltrexone, acamprosate, and disulfiram are reasons to hang up and call the next number 10.
- If you're seizing, hallucinating, confused, or thinking about self-harm, skip the intake call — go to the ER or dial 911, and use SAMHSA's 1-800-662-4357 for immediate non-emergency guidance 8.
- The call itself is the shortest, hardest step: bring the question list, ask what week four looks like, and keep dialing until a program answers with specifics rather than slogans 2.
Before You Pick Up the Phone: What This Call Is Really For
You're probably reading this with a knot in your stomach. Maybe you had your last drink a few hours ago, or maybe you're still deciding if you can stop. Either way, the fact that you're here — researching, not scrolling past — is the first move, and it counts.
Here's what this call is not: a sales pitch you have to sit through, or a moment where a stranger decides your worth. It's a screening conversation. You are interviewing them just as much as they are assessing you. A good outpatient program will expect that and welcome the questions.
What you're really trying to find out in ten or fifteen minutes is whether the program can keep you medically safe during withdrawal and then hand you off — without a gap — into the counseling and medication support that actually treats alcohol use disorder. Detox by itself is not treatment. Every credible clinical guide is clear that withdrawal management has to connect to ongoing care, not end when the shakes stop 2.
The rest of this article gives you the questions to ask, in plain language, and tells you what a solid answer sounds like.
Is Outpatient Detox Actually Safe for You?
Who Ambulatory Withdrawal Management Is Built For
Outpatient detox is not one-size-fits-all. It's designed for a specific kind of drinker: someone whose withdrawal is expected to stay mild, who is medically stable, and who has a safe place to sleep and a person who can check on them.
In clinical language, that means mild withdrawal symptoms and no major risk factors — the group that can be safely treated in an ambulatory setting rather than a hospital bed 5. In plain language: you're shaky, anxious, sweating, maybe not sleeping well, but you're not seizing, not hallucinating, and you're not so sick that you can't hold down water.
A good program will ask you specific things on that first call. How much are you drinking per day, and for how long? When was your last drink? Have you ever had a withdrawal seizure? Are you managing diabetes, heart failure, liver disease, or a serious mental health condition? Do you live with someone sober who can watch you?
If the intake person doesn't ask questions like these, that's information too. A program that skips the screening is not screening you into safety — it's screening you into their schedule.
Red Flags That Mean You Need a Higher Level of Care
Some of what follows may be hard to read. Read it anyway. Knowing where the line is could save your life.
Outpatient detox is not safe for everyone. Worsening symptoms, withdrawal seizures, or signs of delirium tremens require urgent care in a medically managed setting, not a clinic you visit a few times a week 5. The four situations below are the ones most likely to push you out of the ambulatory lane:
- A history of withdrawal seizures. If you've ever had a seizure when you stopped or cut back on drinking, your risk this time is higher. This is not a moment to try to tough it out at home.
- A history of delirium tremens (DTs). Confusion, severe agitation, hallucinations, or a racing heart during past withdrawals mean you need close monitoring, often inpatient.
- Unstable medical or psychiatric conditions. Uncontrolled heart disease, severe liver disease, active suicidal thoughts, or a psychiatric crisis change the math. Withdrawal on top of any of these is not a home project.
- No sober support at home. Someone needs to be there — sober, reachable, and willing to bring you to the ER if things turn. If you're alone, tell the program on the first call.
Ambulatory vs. Medically Managed Inpatient Detox in Maine
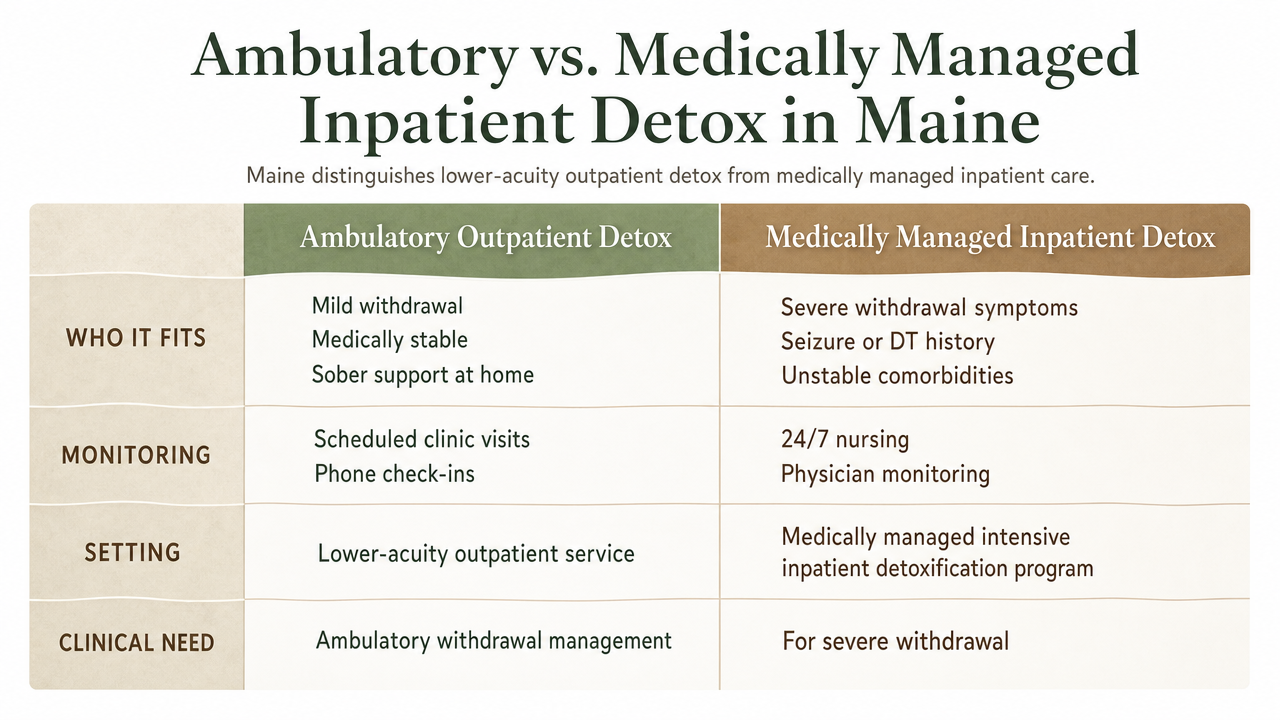
Maine draws a clear line between two different services, and knowing which one you need before you call saves everyone time. State regulation specifically distinguishes medically managed intensive inpatient detoxification programs for people with severe withdrawal symptoms from lower-acuity outpatient services 7. The ASAM guidance for ambulatory withdrawal management fills in the clinical side of that same line 4.
Here's how the two levels of care actually differ:
| | Ambulatory Outpatient Detox | Medically Managed Inpatient Detox ||---|---|---|| Who it fits | Mild withdrawal, medically stable, sober support at home 4| Severe withdrawal symptoms, seizure or DT history, unstable comorbidities 7|| Monitoring | Scheduled clinic visits, phone check-ins between appointments | 24/7 nursing and physician monitoring in a hospital or licensed detox unit || Medications | Benzodiazepines or gabapentin for symptoms; can start naltrexone, acamprosate, or disulfiram for AUD 10| IV medications and rapid dose adjustments as needed || When to escalate | Worsening symptoms, missed doses, seizure, confusion, no safe home 5| Already at the highest level; step down when stable |
If you're a working parent in South Portland who drinks a bottle of wine most nights, has never had a seizure, and has a partner at home, ambulatory is likely a fit. If you're drinking a fifth a day, have shaken through past attempts to stop, or live alone, an inpatient detox followed by outpatient care is the safer route.
Ask the program directly which door you belong at. A trustworthy intake team will tell you — even if the answer means sending you somewhere else first.
The Ten Questions to Ask on the Intake Call
Do You Use a Written Withdrawal Protocol and a Validated Scale Like CIWA-Ar?
This is your opening question, and the answer tells you almost everything about the program's medical seriousness. A written protocol means the clinicians aren't improvising with your nervous system. A validated scale — the most common one is CIWA-Ar, the Clinical Institute Withdrawal Assessment for Alcohol, Revised — means they're scoring your symptoms with the same numbers a hospital would use, not eyeballing you.
Modern standards expect exactly this combination: a standard operating procedure covering diagnosis, validated scoring, level-of-care decisions, and reassessment 1. When the intake coordinator hears "CIWA-Ar" and answers without pausing, that's a good sign. If they say something like, "Our nurse just checks in on you," ask what specifically gets checked and how it's documented.
You don't need to memorize the score ranges. You just need to know that someone is using them, writing them down, and making decisions based on the trend, not a guess.
How Often Will Someone Reassess Me, and Who Decides If I Need to Escalate?
Withdrawal is not a straight line. You can feel steadier at 10 a.m. and worse by dinner. That's why reassessment matters more than any single appointment.
Ask what the first 72 hours actually look like. Daily clinic visits? Phone or video check-ins between visits? A nurse available by text? Written protocols now expect scheduled reassessment across the withdrawal window, not a single intake and a prescription 1.
Then ask the harder question: who has the authority to move you to a higher level of care if your symptoms climb? You want a clear name — a medical director, an on-call physician, a nurse practitioner — not "the team." Escalation is only useful if someone is empowered to pull the trigger fast 5.
A program that treats reassessment as central, not as an afterthought, is one that expects your body to be listened to.
What Medications Do You Use During Withdrawal?
There are two different medication conversations, and they get tangled all the time. This question is about the first one: what will they give you in the acute window, when your body is adjusting to the absence of alcohol.
The honest answer usually includes benzodiazepines, which have long been the standard for calming acute withdrawal symptoms, or gabapentin as an alternative in milder cases 10. Some programs also use adjuncts for blood pressure, nausea, or sleep. Ask which medications they typically prescribe, whether you'll get them at the clinic or fill them at a pharmacy, and how doses are adjusted as you improve.
If the program tells you they don't use any medication for withdrawal — just counseling and encouragement — that is a mismatch for alcohol detox. Untreated withdrawal is not a character-building exercise. It is a medical event, and it deserves medical tools.
Will You Start Me on an AUD Medication Like Naltrexone, Acamprosate, or Disulfiram?
This is the second medication conversation, and it's the one most programs quietly skip. Getting through withdrawal is step one. Staying stopped is a different problem, and there are FDA-approved medications built for it.
Three are approved specifically for alcohol use disorder: naltrexone, acamprosate, and disulfiram 10. Naltrexone is identified as first-line pharmacotherapy with the largest body of evidence behind it, and it can be given as a daily pill or a monthly injection 9. Acamprosate helps steady the brain chemistry that keeps craving loud in the first weeks of sobriety. Disulfiram creates a physical deterrent to drinking. These are not the same category as the benzodiazepines used during withdrawal, and NIAAA is explicit that they serve different purposes 10.
Ask the program directly: do you prescribe naltrexone, acamprosate, or disulfiram, and when in the process do you start them? A real answer sounds like, "We often start naltrexone within the first week, depending on liver labs and your goals." A weak answer sounds like, "We can refer you somewhere for that later."
Think of the full path as a sequence — assessment, withdrawal management, AUD medication, counseling, then relapse prevention and aftercare 2. If a program handles only one box on that path, you'll be assembling the rest yourself while your body is still healing.
What Does the Weekly Schedule Look Like, and Can It Fit Around Work?
You need to know what you're signing up for before you tell your boss anything. Ask for the actual schedule in hours per day, days per week, and total weeks.
In Maine, intensive outpatient programs are typically structured as three to four days a week for about three to four weeks 6. Standard outpatient is lighter. Partial hospitalization is heavier — closer to a full workday, five days a week — and sits between IOP and inpatient care. Some programs offer morning tracks, some run in the evening, some do both.
If you work days, ask about an evening IOP. If you're caring for kids after school, ask about morning groups. If you travel for work, ask what telehealth options exist for check-ins between in-person visits.
Then ask what happens if you miss a session because a client meeting runs long or your kid gets sick. A program built for working adults will have an answer that isn't "we discharge you."
What Happens After the Acute Withdrawal Window Closes?
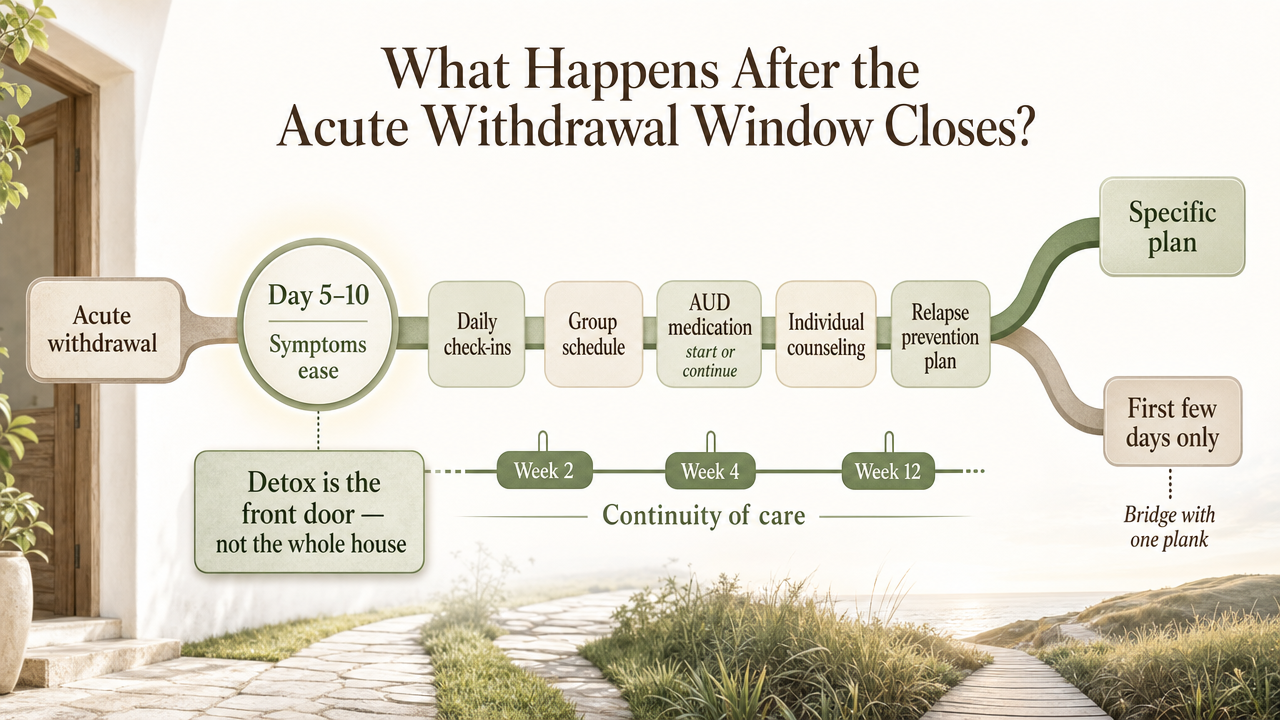
Somewhere between day five and day ten, the shaking stops and the harder work starts. Ask what the program does at that hinge point, because this is where a lot of people fall through a gap.
Detox that ends when symptoms end is not treatment. Every credible clinical guide treats withdrawal management as the front door of care, not the whole house 2. What you want to hear is a specific plan: you'll move from daily check-ins into a group schedule, you'll start or continue AUD medication, you'll begin individual counseling, and someone will help you build a relapse prevention plan.
If the program can describe week two, week four, and week twelve without stumbling, that's continuity. If they can only describe the first few days, you're being sold a bridge with one plank. NIAAA's guidance to patients puts it plainly: treatment for alcohol problems is a longer arc that pairs counseling with medication support 3.
How Do You Handle Co-Occurring Anxiety, Depression, or Trauma?
For a lot of people, drinking has been the tool that quieted something underneath. When the alcohol goes, whatever it was covering shows up in the room. That's not weakness. That's physiology and biography.
Ask the program how they handle co-occurring conditions. Do they have clinicians who treat anxiety, depression, PTSD, or trauma histories alongside the substance use — not in a separate building, and not "once you're stable"? Do they use approaches like CBT, DBT, motivational interviewing, and trauma-informed care as part of the same treatment plan?
Updated standards expect programs to address concurrent conditions rather than pretend they'll sort themselves out 1. If the intake person says something like, "You'd need to see your own therapist for the anxiety stuff," that split will almost always cost you continuity. You want one team, one chart, one plan.
Who Do I Call at 2 a.m. If Symptoms Get Worse?
This question sounds simple. The answer separates the safe programs from the ones you should keep looking past.
Ask for the exact number, who answers it, and what hours it's staffed. Is it a nurse line? An on-call clinician? A voicemail that gets returned in the morning? Voicemail is not an answer at 2 a.m. Worsening symptoms, confusion, or a seizure need urgent care in real time, not the next business day 5.
A responsible outpatient program will also tell you plainly when to skip them and call 911 or go to the nearest emergency room — for a seizure, severe confusion, chest pain, or a fever with heavy sweating. If they hedge on that, that's the hedge that matters. If they give you a direct after-hours contact and a clear ER trigger list, you have a real safety net.
What Do You Actually Charge, and What Will My Insurance Cover?
Money stress is not a distraction from recovery. It's a relapse risk. Get the numbers before you start.
Ask what insurance plans they accept, whether they're in-network or out-of-network for yours, and what your likely out-of-pocket cost is for each level of care. Ask if the program will run a verification of benefits before your first appointment so you're not surprised by a bill. Ask about self-pay rates if you're uninsured, and whether they offer sliding scale or payment plans.
Then call your insurance directly. Ask about deductibles, co-pays for outpatient behavioral health, and whether AUD medications like naltrexone are covered under your pharmacy benefit. Two calls now save weeks of billing anxiety later.
A program that answers cost questions clearly, in writing, is one that respects your ability to plan. Vague answers here often mean vague answers everywhere.
What Happens If I Drink During Treatment?
Ask this one out loud, even if it feels like admitting something. The answer tells you whether the program understands the disease they treat.
A relapse during outpatient detox is not a moral failure. It's clinical information. It usually means the plan needs to be adjusted — more support, different medication, sometimes a step up to a higher level of care for a few days. What you want to hear is that the program responds with a clinical review, not a discharge letter.
Ask directly: do you drug or breath test, and what happens with the results? Do you kick people out for using? Do you adjust the treatment plan and keep going? Programs grounded in evidence treat lapses as part of the arc of recovery, not as a violation to punish. If the answer sounds punitive, keep dialing. Shame has never been a treatment.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
What a Good Answer Sounds Like (and What Should Make You Hang Up)
"We use CIWA-Ar scoring at each visit, our medical director reviews the trend daily, and we typically start naltrexone in week one if your labs support it" 9.
A weak call sounds vague. Lots of warmth, no specifics. "Don't worry, we take care of everything." No mention of a written protocol. No answer for who's on call after hours. No plan for what happens after withdrawal settles. When you ask about naltrexone, acamprosate, or disulfiram, they change the subject 10.
Hang-up signals worth trusting: pressure to commit before an assessment, a refusal to discuss cost, discharge threats if you drink during treatment, or a promise that detox alone will fix things. Detox is the front door, not the house 2.
If something feels off, it probably is. Thank them, hang up, and call the next number on your list.
If You're in Crisis Before You Finish Reading This
If you're not in medical danger but you need to talk to someone right now — tonight, this hour — SAMHSA's National Helpline is free, confidential, and staffed 24/7 at 1-800-662-4357 8. They can help you figure out what level of care you actually need and point you toward local options in Maine.
Making the call is not the finish line. It's the first honest step, and you're already taking it.
Making the Call
Making the call is the hardest sentence you'll say all week. It's also the shortest one in this whole process.
You don't need a script memorized. You need this article on your screen, a pen, and ten minutes. Ask about the withdrawal protocol, the CIWA-Ar scoring, the after-hours number, and whether they'll start you on naltrexone, acamprosate, or disulfiram when the time comes 10. Ask what week four looks like, not just week one 2.
If the first program isn't right, call the next one. If you're in South Portland, ask about evening IOP so work doesn't have to know before you're ready. Coastal Recovery Partners is one option in the area, and there are others — what matters is that someone answers your questions with specifics, not slogans.
You're already doing the thing most people don't. Keep going.
Frequently Asked Questions
How long does outpatient alcohol detox usually take?
The acute withdrawal window is typically five to seven days, with the roughest stretch in the first 72 hours. After that, most people step into an intensive outpatient program that runs three to four days a week for about three to four weeks in Maine 6. The full arc of care lasts longer.
Can I keep working during outpatient detox?
Often, yes — that's part of why outpatient exists. Many programs offer morning or evening tracks so you can keep your job. That said, the first few days can be physically hard, so plan for reduced hours or a short leave at the start. Ask the intake team what a realistic first week looks like for someone in your role.
What's the difference between detox and treatment for alcohol use disorder?
Detox handles the acute withdrawal — the shaking, anxiety, and physical symptoms when alcohol leaves your system. Treatment for alcohol use disorder is longer and includes counseling, relapse prevention, and FDA-approved medications like naltrexone, acamprosate, or disulfiram 10. Detox is the front door. The building behind it is where the actual work of staying stopped happens 2.
Will I be given medication during outpatient detox?
Usually, yes. Benzodiazepines are the standard for calming acute withdrawal, and gabapentin is sometimes used for milder cases 10. A well-run program will also talk with you about starting a longer-term AUD medication once you're stable — naltrexone is identified as first-line pharmacotherapy with the strongest evidence base 9. If a program tells you no medication is used, keep looking.
How do I know if outpatient detox isn't safe for me?
Ambulatory detox is built for mild withdrawal with no major risk factors 5. If you've had a withdrawal seizure, delirium tremens, unstable heart or liver disease, active psychiatric crisis, or no sober person at home, you likely need medically managed inpatient detox first 7. Say all of that on the intake call. A good program will route you to the right level of care.
What should I do if I can't reach a program right now?
Call SAMHSA's National Helpline at 1-800-662-4357. It's free, confidential, and staffed 24/7, and they can point you toward local Maine options 8. If you're having a seizure, severe confusion, chest pain, or thoughts of hurting yourself, call 911 or go to the nearest emergency room instead.
References
- VHA Notice 2024-09, Alcohol Withdrawal Management. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=11928
- Quick Guide For Clinicians Based on TIP 45—Detoxification and Substance Abuse Treatment. https://nida.nih.gov/sites/default/files/samhsa_detoxification_and_substance_abuse_treatment.pdf
- Treatment for Alcohol Problems: Finding and Getting Help. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
- The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management Pocket Guide. https://www.samhsa.gov/resource/ebp/asam-clinical-practice-guideline-alcohol-withdrawal-management-pocket-guide
- Alcohol Withdrawal Syndrome - StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK441882/
- Substance Use Disorder Treatment - Maine.gov. https://www.maine.gov/dhhs/obh/support-services/substance-use-disorder-services/treatment-services
- 14-118 C.M.R. ch. 5, § 19 - SUBSTANCE ABUSE TREATMENT .... https://www.law.cornell.edu/regulations/maine/14-118-C-M-R-ch-5-SS-19
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- Alcohol Use Disorder (AUD) - VA Pharmacy Benefits Management. https://www.pbm.va.gov/PBM/AcademicDetailingService/Documents/508/10-1530_AUD_ClinicianGuide_508Conformant.pdf
- Medications Development Program. https://www.niaaa.nih.gov/medications-development-program


