
What to Expect From Drug and Alcohol Rehab

Understanding Drug and Alcohol Rehab Treatment Levels and Placement
How Treatment Intensity Is Determined
When navigating drug and alcohol rehab, a practical tool often used to determine the right level of care is the ASAM Criteria checklist. This assessment evaluates six core dimensions: substance use history (including intoxication and withdrawal risk), biomedical conditions, emotional status, readiness for change, potential for relapse, and recovery environment. At Coastal Recovery Partners in South Portland, Maine, our clinical team uses these dimensions to match individuals with outpatient, intensive outpatient (IOP), partial hospitalization (PHP), or residential treatment settings, always aiming for the least restrictive option that meets safety and therapeutic needs.3
ASAM Criteria Dimensions for Treatment Placement
Treatment intensity is rarely decided by a single factor. Clinical teams weigh acute withdrawal symptoms, co-occurring disorders, social support, and recent relapse history. For example, someone with stable housing and good family support may benefit from an intensive outpatient program, while those facing severe withdrawal or unmanaged mental health symptoms might require partial hospitalization.
"Matching the patient to the correct level of care from day one is the cornerstone of effective addiction treatment, reducing the risk of early dropout and setting a foundation for long-term recovery."
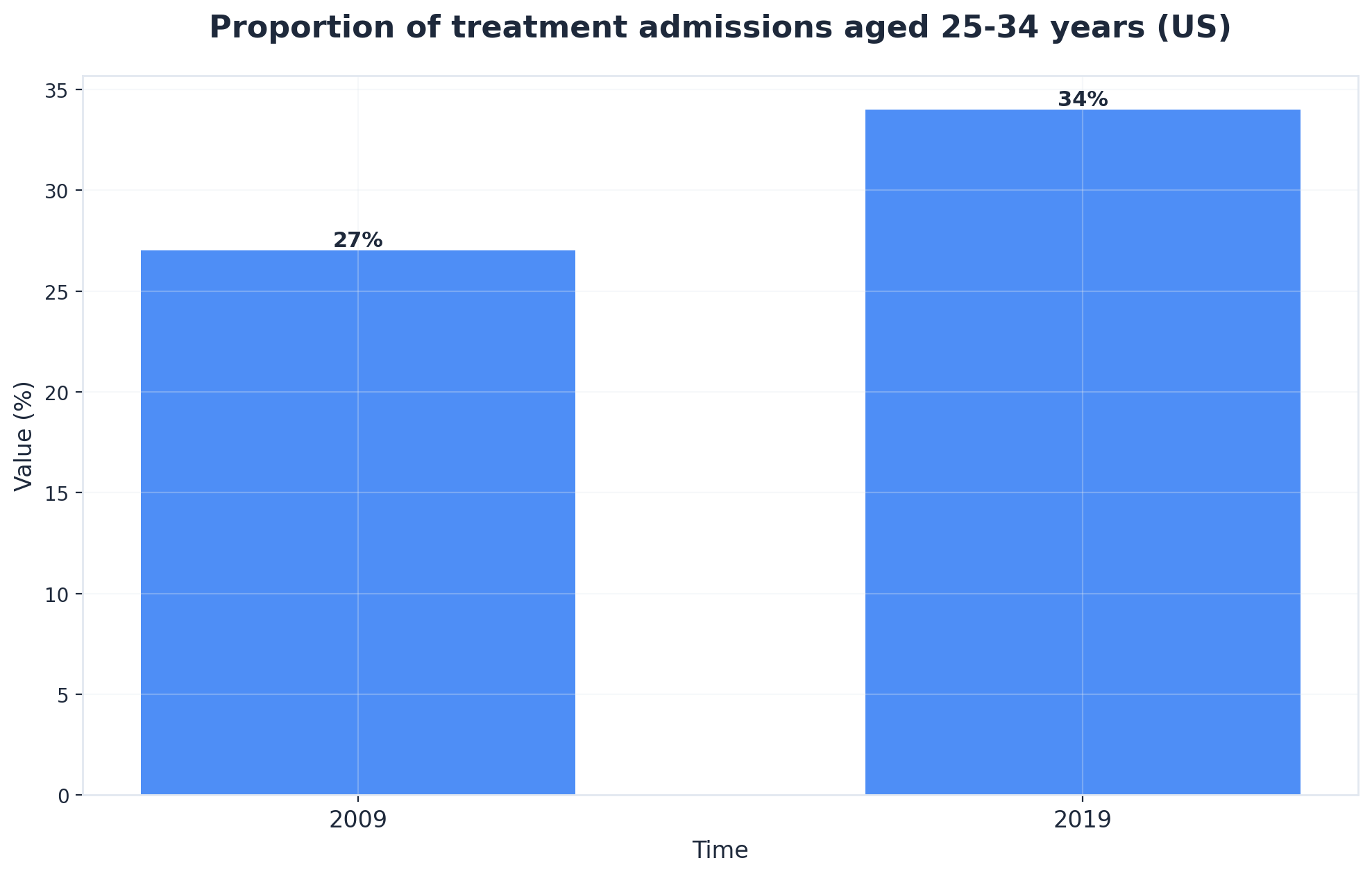
This approach works best when professionals need to balance work with treatment or are transitioning from higher levels of care. Assessment tools typically require a 60- to 90-minute intake, gathering information from both the individual and—with consent—collateral sources. Recognizing that 45% of individuals in treatment also have co-occurring mental health conditions, integrated assessment is now standard practice.4
Outpatient vs. Residential Care Models
Selecting between outpatient and residential care models often begins with a practical placement matrix. This tool helps professionals weigh daily structure needs, medical supervision, environmental stability, and personal obligations. Outpatient treatment allows individuals to maintain work and family responsibilities while participating in structured therapy several days per week. Costs for outpatient care typically range from $1,000 to $5,000 per month depending on intensity, making it a cost-effective alternative to residential stays.
These programs—ranging from standard outpatient to intensive outpatient or partial hospitalization—are best suited for those with stable living environments and moderate symptom acuity. Research shows comprehensive outpatient care can result in 40-60% improvement in substance use outcomes at one-year follow-up.2
Residential (inpatient) care, by contrast, provides 24-hour support in a controlled setting. This option is recommended when withdrawal risks are high, home environments are unstable, or when previous outpatient attempts have not led to sustained change. Consider this method if acute medical or psychiatric supervision is required. Residential programs tend to be more resource- and time-intensive, often requiring 30 to 90 days of on-site participation and a pause from outside responsibilities.
This distinction is especially relevant for first-time treatment seekers balancing professional commitments. Outpatient models prioritize flexibility, while residential care provides intensive immersion for those needing a higher level of stability. Comparing these approaches clarifies what individuals can expect when exploring care options. Next, attention turns to the therapeutic methods and interventions that shape recovery outcomes.
Core Drug and Alcohol Rehab Treatment Components and Therapies
Evidence-Based Behavioral Interventions
A practical tool for mapping the behavioral therapies used in treatment is the "Therapy Modalities Grid." This chart outlines which interventions are standard at each treatment level. At Coastal Recovery Partners, our clinical programming relies heavily on these evidence-based practices to ensure high-quality care.
- Cognitive Behavioral Therapy (CBT): Focuses on identifying thought patterns that drive substance use, equipping individuals with actionable coping strategies.
- Dialectical Behavioral Therapy (DBT): Adds skills for emotional regulation and distress tolerance, especially valuable for those managing intense emotions alongside addiction.
- Motivational Interviewing: A conversational technique that builds readiness for change by drawing out personal motivation and resolving ambivalence.
- Relapse Prevention Therapy: Teaches practical approaches to high-risk situations and long-term recovery planning.
Research consistently shows that combining these evidence-based techniques leads to better outcomes than any single approach alone. This strategy suits organizations that aim to provide holistic care for professionals facing complex challenges. Therapy sessions may be scheduled in individual, group, or family formats, with frequency tailored to clinical need—ranging from two to ten hours weekly, depending on program intensity.6
Engagement in these interventions is linked to improved retention, which remains the strongest predictor of sustained recovery. For first-time treatment seekers, understanding the therapeutic landscape sets clear expectations for the work ahead. Next, the discussion turns to how medication-assisted treatment integrates with behavioral therapy to support lasting change.7
Medication-Assisted Treatment Integration
A practical decision tool for medication-assisted treatment (MAT) integration is the "MAT Suitability Checklist." This resource guides professionals in evaluating whether medications—combined with counseling—fit a client’s clinical profile, substance use history, and recovery goals. MAT refers to the use of FDA-approved medication alongside behavioral therapies to address substance use disorders, most commonly for opioid or alcohol dependence.
View the MAT Suitability Checklist
- Does the individual have a history of chronic relapse?
- Are severe withdrawal symptoms or cravings present?
- Have behavioral interventions alone proven insufficient?
- Is there a co-occurring medical condition that requires coordinated care?
MAT is increasingly recognized as a gold standard in care, especially for clients with opioid use disorder or those at heightened risk of relapse. MAT helps reduce cravings and withdrawal symptoms, making it easier for individuals to remain engaged in therapy and daily responsibilities. Under the guidance of our Medical Director, Dr. Brian K. Adler, Coastal Recovery Partners coordinates MAT programs that combine medication with robust therapeutic support.
Research indicates that combining MAT with counseling can reduce illicit opioid use by 50% or more, and improve retention compared to therapy alone. Opt for this framework when patients have a history of chronic relapse, severe withdrawal, or have not achieved stability with behavioral interventions alone. Implementing MAT requires medical oversight—typically involving regular physician visits, urine drug screens, and medication management appointments.8
Time commitments vary, but initial stabilization may require weekly appointments, tapering to monthly as recovery progresses. Insurance coverage for MAT has expanded in recent years, although prior authorization and formulary limitations may apply. MAT is not a standalone solution; successful integration depends on coordination with counseling and relapse prevention planning.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Dual Diagnosis and Trauma-Informed Care
Addressing Co-Occurring Mental Health Needs
A practical tool for managing co-occurring mental health needs is the "Integrated Symptom Monitoring Checklist." This assessment is used throughout treatment to track both substance use and mental health symptoms—such as anxiety, depression, or PTSD—ensuring interventions remain responsive to evolving client needs. For example, clinicians might instruct a patient to log daily mood scores in a secure portal or press Submit on a weekly digital assessment.
// Example Symptom Log Entry
Dual diagnosis refers to the presence of both a substance use disorder and a mental health condition, a situation found in roughly 45% of individuals seeking addiction treatment. Integrated care works best when clinical teams collaborate across disciplines, combining psychiatric evaluation, medication management, and evidence-based psychotherapy.4
For instance, a professional experiencing alcohol dependence and major depression may benefit from a care plan including cognitive-behavioral therapy, targeted medication, and regular psychiatric check-ins. This path makes sense for organizations that wish to address the whole person, not just the addiction, and is particularly relevant for working adults balancing demanding schedules with emotional challenges.
Prioritizing dual diagnosis treatment is linked to improved engagement and reduced relapse rates compared to treating each issue in isolation. Resource needs for integrated care include access to mental health clinicians, medication prescribers, and ongoing outcome measurement. Time investments may range from several hours weekly for therapy and medication management to periodic multidisciplinary case reviews.4
Trauma-Responsive Treatment Protocols
A practical framework for trauma-responsive care is the "Safety and Empowerment Protocol Checklist." This tool guides clinical teams in creating environments where clients feel secure, respected, and actively involved in their own treatment planning. Trauma-informed care recognizes that many individuals seeking rehab have a history of adverse experiences—such as abuse, neglect, or violence—that can influence both substance use and recovery trajectories.
Trauma-responsive protocols prioritize nonjudgmental communication, predictable routines, and clear consent processes for every intervention. Consider this route if treating professionals who may mask trauma symptoms or minimize their impact due to workplace expectations. Protocols might include dedicated trauma screening at intake, regular staff training in de-escalation and grounding techniques, and flexible scheduling to accommodate emotional triggers.
At Coastal Recovery Partners, explicit trauma-informed protocols are woven into every level of care, ensuring that therapies are delivered safely. Research shows that integrating trauma-informed practices in addiction treatment contributes to higher engagement and improved outcomes, particularly for those with dual diagnosis or chronic relapse histories.4
Resource requirements for trauma-responsive care include ongoing staff education, access to trauma-specific therapies, and multidisciplinary team collaboration. Time investments may involve additional assessment hours and frequent case consultations. Building trauma-responsive protocols lays the groundwork for understanding how treatment duration and engagement timelines affect long-term success, which will be explored next.
Treatment Duration and Success Factors
Engagement Timelines and Retention Drivers
A practical tool for monitoring engagement is the "Retention Milestone Calendar." This calendar sets clear participation goals to help both individuals and clinical teams visualize progress across the critical first 30, 60, and 90 days.
- Day 30: Establish therapeutic alliance, stabilize withdrawal symptoms, and complete initial treatment planning.
- Day 60: Deepen engagement in group therapy, begin applying coping skills in real-world settings, and adjust MAT if necessary.
- Day 90: Solidify relapse prevention strategies, transition to lower intensity care (e.g., from PHP to IOP), and begin formal aftercare planning.
Research shows that remaining engaged for 90 days or longer significantly increases the likelihood of sustained recovery, with outcomes improving measurably compared to shorter stays. Retention drivers include early therapeutic alliance, flexible scheduling, and regular outcome tracking.2
This approach is ideal for organizations supporting professionals who must coordinate treatment with career or family obligations. Consistent communication about progress, along with adapting interventions to address emerging needs, keeps engagement high. For instance, programs offering evening sessions or virtual group options often see stronger retention among working adults.
Time investment varies, but most outpatient schedules involve 6–12 hours of structured treatment per week during the first phase, tapering as stability improves. Prioritize this when working with first-time treatment seekers, as ongoing participation is the strongest predictor of positive outcomes.7
Aftercare Planning and Alumni Support
A practical tool for ensuring ongoing recovery is the "Aftercare Roadmap Planner." This structured guide helps professionals and clients map out a personalized plan that includes support groups, continued therapy, scheduled check-ins, and peer-driven alumni networks. Aftercare planning begins before discharge and typically includes concrete milestones: joining a relapse prevention group, establishing weekly or monthly alumni meetings, and setting up contact with a recovery coach or sponsor.
This solution fits organizations committed to long-term outcomes, as research consistently links aftercare engagement to lower relapse rates and improved sustained recovery. For first-time treatment seekers, aftercare is not an optional add-on—it's a core extension of the treatment process. Alumni support programs offer ongoing connection and accountability, which is especially valuable for professionals returning to high-stress environments.7
Resource requirements for aftercare include access to ongoing group sessions, digital communication tools for alumni, and staffing for periodic outreach. Time investment varies: most individuals dedicate 1–3 hours weekly to aftercare in the first six months post-discharge, with the option to taper as stability grows.
Coastal Recovery Partners emphasizes robust alumni support and aftercare to ensure you remain connected to a recovery community. This method works when your organization serves adults balancing recovery with demanding careers, as ongoing support is a proven driver of lasting success.7
Your Path Forward: Taking the Next Step
Outpatient treatment models have evolved to address a critical gap in addiction care: providing clinical rigor while preserving professional and personal continuity. For individuals maintaining careers, family responsibilities, or community connections, structured outpatient programs deliver evidence-based interventions without requiring residential placement. This approach supports recovery while minimizing disruption to established routines and obligations.
Coastal Recovery Partners structures its clinical programming across three levels of care to match treatment intensity with individual need. The Partial Hospitalization Program (PHP) provides the highest level of outpatient intervention, typically meeting five to six days weekly for comprehensive therapeutic engagement. The Intensive Outpatient Program (IOP) offers structured treatment three to five days per week, balancing clinical support with professional obligations. Standard Outpatient (OP) services provide ongoing maintenance care for sustained recovery.
All programs operate on flexible schedules—morning, afternoon, and evening sessions—designed specifically to accommodate working professionals and those with family commitments. This scheduling framework enables continuity of care without requiring extended leave from employment or significant lifestyle disruption. Under the leadership of Clinical Director and CEO Spencer Josey, our team ensures that every treatment plan is customized to your unique circumstances.
Clinical assessment begins with comprehensive evaluation that identifies substance use patterns, co-occurring mental health conditions, and individual treatment needs. Treatment plans integrate evidence-based modalities including Cognitive Behavioral Therapy, Dialectical Behavioral Therapy, and motivational interviewing, supplemented by medication-assisted treatment when clinically indicated. The trauma-informed care model addresses underlying factors that contribute to substance use, while care coordination services streamline insurance navigation and treatment planning.
Selecting an appropriate treatment program requires understanding both clinical needs and practical considerations around scheduling, insurance, and program structure. Coastal Recovery Partners provides consultation to help individuals identify the level of care that aligns with their current situation and recovery goals. Information about program options, insurance verification, and treatment planning is available through direct contact with the clinical team.
Remember that recovery is a journey of rebuilding trust—in yourself, in others, and in the process of healing. If you are ready to explore your options, reach out to Coastal Recovery today. We're here to help guide you toward a future defined not by your past, but by your resilience and hope.

Frequently Asked Questions
How do I choose between different outpatient program intensities?
Choosing between standard outpatient, intensive outpatient (IOP), and partial hospitalization (PHP) programs in drug and alcohol rehab typically starts with a structured assessment—such as the ASAM Criteria—which evaluates factors like withdrawal risk, co-occurring health conditions, and daily responsibilities. Opt for standard outpatient when symptoms are mild and work or family obligations are steady. IOP is well-suited for moderate severity, providing more frequent therapy while maintaining outside commitments. PHP offers the highest outpatient intensity for those needing daily support but not full residential care. This approach is ideal for professionals seeking flexibility without sacrificing clinical rigor. Discuss with your clinical team to match intensity to current needs.3
What does treatment cost and what insurance coverage can I expect?
Treatment costs for drug and alcohol rehab can vary widely depending on program type, duration, and location. Outpatient programs are generally less expensive than residential or partial hospitalization options, but the actual dollar amounts will differ based on insurance contracts, clinical needs, and regional rates. Most commercial insurance plans, as well as Medicaid and Medicare, now cover evidence-based addiction treatment—including outpatient, intensive outpatient, and medication-assisted options—though prior authorization or co-pays may apply. This approach is ideal for organizations supporting professionals who need predictable budgeting and insurance navigation. It’s important to verify coverage and network status with your insurer before starting, as coverage specifics and out-of-pocket costs can differ. If clients are uninsured, state and federal assistance programs are available to help reduce financial barriers to care.1,12
Can I continue working while attending outpatient treatment?
Yes, many professionals are able to continue working while participating in outpatient drug and alcohol rehab. Outpatient programs are specifically structured to allow flexibility, with sessions commonly scheduled in the mornings, afternoons, or evenings to accommodate work commitments. Typical time investments range from 6 to 12 hours per week, depending on the program intensity and individual clinical needs. This approach works best when a person has a supportive work environment and stable daily routine, as maintaining employment can reinforce structure and motivation during recovery. Open communication with your employer about scheduling—if comfortable—can further ease the process and minimize work-life disruptions.2
What happens if I relapse during or after completing treatment?
Relapse is not uncommon during or after completing drug and alcohol rehab, and it does not mean treatment has failed. Addiction is considered a chronic, relapsing condition that often requires ongoing management and adjustment of care strategies. If a relapse occurs, best practice involves promptly reaching out to your clinical team to reassess triggers, update the treatment plan, and strengthen support structures. This path makes sense for professionals who experience increased stress or life changes after discharge. Many programs offer rapid re-engagement options, including intensified outpatient sessions or renewed medication management. Research shows that returning to treatment after a relapse can still lead to sustained recovery, especially when combined with aftercare and ongoing therapeutic support.7,10
How do I know if I need medication as part of my treatment plan?
Determining if medication is right for your drug and alcohol rehab plan starts with a collaborative assessment involving your clinical team. Medications such as buprenorphine, methadone, or naltrexone are typically considered when there is a history of opioid or alcohol dependence, repeated relapse, or severe withdrawal symptoms. This method works when behavioral therapies alone have not led to stable progress, or when cravings and physical symptoms remain barriers to engagement. The decision also factors in co-occurring health issues, current medications, and individual recovery goals. Professional evaluation, rather than self-diagnosis, ensures medication-assisted treatment is matched to your unique needs and supports the safest, most effective path forward.8
What role does family involvement play in the treatment process?
Family involvement is a key driver of successful outcomes in drug and alcohol rehab. When loved ones participate in therapy sessions, educational workshops, or support groups, individuals are more likely to remain engaged and achieve lasting change. This approach works best when families are educated about addiction as a medical condition and equipped with communication and boundary-setting skills. For professionals, family involvement can provide emotional support and accountability while also helping to address workplace pressures or stigma that may impact recovery. Research shows that active family participation is linked to higher retention rates and reduced risk of relapse, reinforcing the collaborative nature of the treatment process.2,7
References
- SAMHSA Treatment Services Locator & Research Data. https://www.samhsa.gov/data-research/treatment
- Principles of Drug Addiction Treatment: A Research-Based Guide. https://www.nida.nih.gov/publications/principles-drug-addiction-treatment
- American Society of Addiction Medicine (ASAM) Criteria for Treatment Placement. https://www.asam.org/resources/the-asam-criteria
- National Institute of Mental Health: Substance Use and Co-occurring Mental Illness. https://www.nimh.nih.gov/health/topics/substance-use-and-co-occurring-mental-illness
- CDC: Drug Overdose Prevention. https://www.cdc.gov/drugoverdose/prevention/index.html
- NIDA: Therapeutic Research on Addiction Treatment. https://www.drugabuse.gov/publications/research-reports/therapeutics-research-international-consortium-addiction-treatment-genetics
- NCBI/PubMed: Substance Use Disorder Treatment Effectiveness and Retention. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6335826/
- Peer-Reviewed Research: Medication-Assisted Treatment Outcomes. https://pubmed.ncbi.nlm.nih.gov/21977682/
- SAMHSA Technical Assistance Publication: Enhancing Motivation for Change. https://store.samhsa.gov/product/TIP-35-enhancing-motivation-for-change-in-substance-abuse-treatment/PEP05-0095
- American Psychiatric Association: Understanding Addiction. https://www.psychiatry.org/patients-families/addiction/what-is-addiction



