
Practical Recovery Skills for Long-Term Sobriety

Key Takeaways
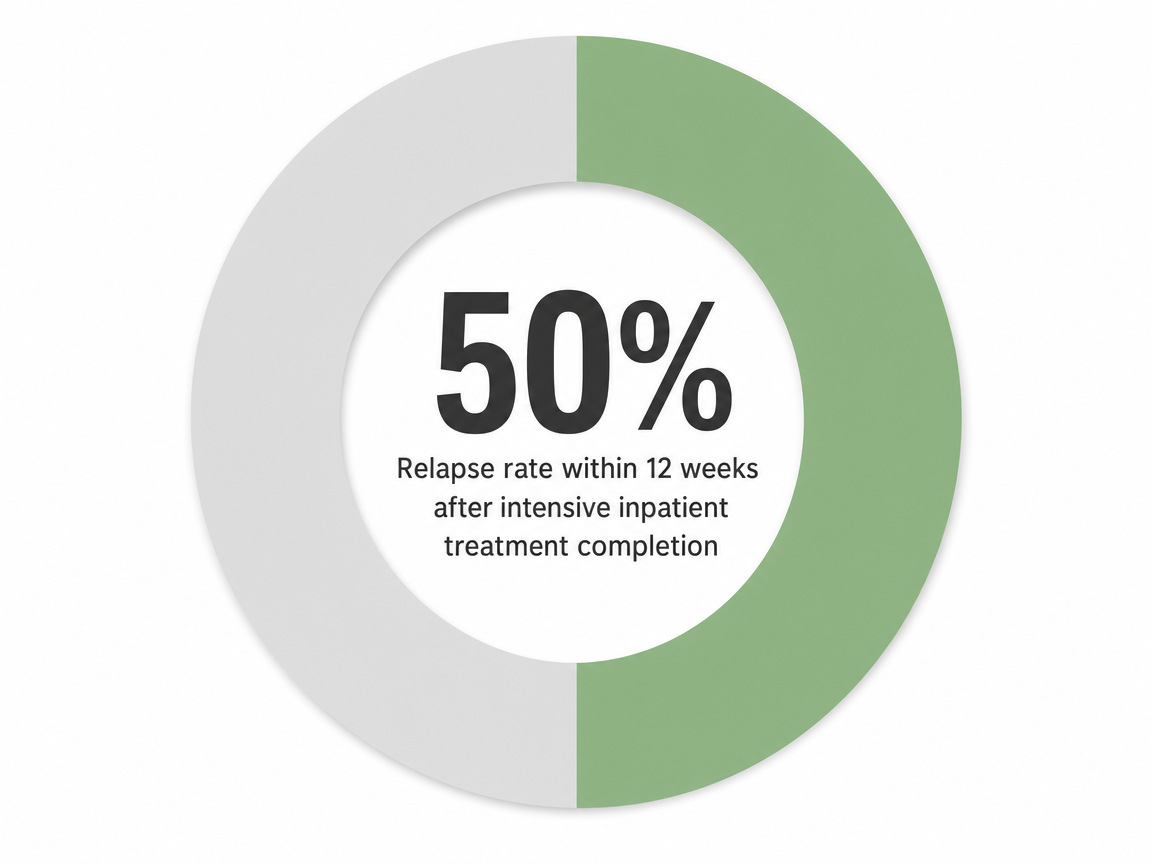
- The first 12 weeks after treatment are a practice window, not a waiting room — roughly half of people relapse in this stretch, so daily skill use matters more than dramatic moments 1.
- Relapse moves through three stages — emotional, mental, then physical — and intervening upstream at HALT signs or romanticizing thoughts is far easier than stopping a hand already moving 2.
- Cognitive restructuring, DBT distress tolerance, urge surfing, and HALT self-checks form the core skill families with the strongest evidence base for staying sober 8, 5, 7.
- Skills hold up only when paired with connection, lifestyle repair, medication when indicated, and aftercare lasting 6 months or longer — and recurrence is data for adjusting treatment, not a verdict 14, 12.
The First 12 Weeks Are a Skills Window, Not a Waiting Room
You finished treatment. The schedule loosened. The group room is a memory now, and the question on Monday morning is a quiet one: what do I actually do today?
Here's the part nobody softens enough. Roughly 50% of people relapse within 12 weeks of completing intensive inpatient treatment, and that window is exactly when daily structure thins out 1. The number isn't meant to scare you. It's meant to tell you something useful: the first three months after stepping down aren't a victory lap, and they aren't a waiting room either. They're a practice room.
Think of recovery skills the way a musician thinks about scales. Nobody plays scales because the moment is dramatic. You play them on Tuesday at 9 a.m. when nothing is happening, so that when something does happen, your hands already know where to go. Cognitive restructuring, urge surfing, the phone call you make before you need to make it — these are scales. They feel small. They are not small.
If you're reading this 3 weeks out or 18 months out, the work is the same shape: notice early, intervene early, stay connected. The rest of this guide walks you through the specific skills that hold up when life gets loud, organized around the stage of recovery you're actually standing in — not a flat list of tips that ignores where you are.
You've already done the hardest part, which was starting. Now you're learning how to keep it.
Reading the Three-Stage Relapse Arc Before It Reaches Your Hand
Emotional Relapse: When You Stop Taking Care of Yourself
The first stage doesn't look like relapse. That's what makes it dangerous.
Emotional relapse is the stretch where you're not thinking about using — you're just slowly stopping the things that keep you well. You skip the meeting because you're tired. You stop returning your sponsor's texts. You eat lunch at your desk for the third day in a row. Sleep gets weird. You feel a low irritation you can't quite name, and when someone asks how you're doing, you say "fine" a little too fast 2.
The clinical signs are quieter than the language suggests: poor self-care, isolating, suppressing feelings, attending recovery activities but not engaging in them 2. None of these alone means you're in trouble. Stacked together for a week, they mean your defenses are thinning.
The intervention here is small and almost embarrassing in its simplicity. Eat. Sleep. Call one person. Go to the meeting and actually speak. You don't need a breakthrough. You need to refuse the drift. This is where recovery skills earn their keep — not in the dramatic moment, but in the boring Tuesday when you choose to take care of yourself before you have a reason to 1.
Mental Relapse: The Argument Inside Your Head
If emotional relapse is silence, mental relapse is noise. There's a part of you that wants to use, and a part of you that doesn't, and they're starting to argue out loud.
You catch yourself romanticizing — remembering the warmth of the first drink, not the 2 a.m. shame. You think about the people you used with and feel a strange tug of nostalgia. You start bargaining: maybe just on weekends. Maybe just this one time, for the wedding. You drive past the old neighborhood for no reason. You look up an old number. You start planning around it without admitting you're planning 2, 1.
This is the stage where the three-stage arc — emotional, mental, physical — becomes a tool you can actually use. Knowing where you are matters. The early signs of emotional relapse (HALT: hungry, angry, lonely, tired, plus isolating and skipping recovery activities) sit upstream of mental relapse signs (romanticizing past use, lying, planning around people or places), which sit upstream of physical relapse 2, 1. Each stage has a self-check. Each stage has a window.
When you notice the argument, the skill is to interrupt it, not to win it. Tell someone the thoughts out loud — a sponsor, a therapist, a friend who knows. Spoken cravings lose volume. The fantasy needs privacy to grow. Take it away.
Physical Relapse: Why Intervening Here Is Already Late
Physical relapse is the drink, the pill, the line. By the time you're standing at this stage, the work of prevention has already been outrun.
That isn't a moral statement. It's a mechanical one. Most people who use again describe a moment of opportunity — a few unsupervised minutes, a familiar place, a stress that landed harder than expected — and a decision that felt sudden but wasn't. The decision was assembled over days or weeks of unaddressed emotional and mental relapse 1.
If you're already past this point, that's a different conversation, and it's one this article will come back to. Recurrence is not a verdict. But the goal of learning the arc is so you can act before your hand moves.
The Core Skill Families That Actually Hold Up
Cognitive Restructuring: Catching the Thought Before It Catches You
A craving rarely shows up as a craving. It shows up as a thought that sounds reasonable.
I've had a brutal week. I've earned a break. One drink isn't using. Everyone else at the table will be drinking — it'll be weird if I don't. The thought feels like yours. It feels like logic. That's the trap.
Cognitive restructuring is the skill of catching the thought, naming it, and testing it before you act on it. It comes out of cognitive behavioral therapy, which has the strongest evidence base of any psychological treatment for substance use disorders 8. In Marlatt's relapse prevention model, restructuring sits alongside skills training and lifestyle balance as one of the three pillars that target the actual antecedents of relapse — not the substance itself, but the thinking that opens the door 3.
The practice is simpler than it sounds. When a thought spikes, you ask three questions:
- Is this true?
- What's the evidence on the other side?
- What would I tell a friend who said this out loud?
I've earned a break becomes I'm exhausted, and a drink would cost me more than it would give me. What I've earned is sleep, a real meal, and a phone call to someone who gets it.
You're not arguing with yourself. You're slowing the thought down enough to see it. Done a few times a day, this becomes muscle memory. The thought still arrives. It just stops driving.
Distress Tolerance and Emotion Regulation, Borrowed From DBT
Some feelings can't be reasoned with. They have to be ridden out.
That's the territory dialectical behavior therapy was built for — the emotional weather that's too big for cognitive restructuring alone. DBT teaches two skill clusters that matter especially for recovery: distress tolerance (getting through a hard moment without making it worse) and emotion regulation (lowering the baseline so fewer moments become hard in the first place). A randomized trial of standalone DBT skills training found that participants with co-occurring substance use and mental health conditions were more likely to achieve full SUD remission, with measurable gains in skills use over standard care 5. If you carry anxiety, depression, PTSD, or anything else alongside the addiction, this is your toolkit.
A few skills worth knowing by name:
- TIPP
- when distress is at a 9 out of 10, you change your body chemistry fast. Cold water on the face, paced breathing (longer exhale than inhale), brief intense exercise. It buys you fifteen minutes of clearer thinking.
- Opposite action
- when the urge is to isolate, you reach out. When the urge is to lash out, you soften your voice. You act against the emotion's pull, not because the feeling is wrong, but because the action it suggests would cost you.
- Radical acceptance
- this hour is hard. You don't have to like it. You just have to stop fighting that it's happening, because the fighting is what eats your energy.
None of these fix the feeling. They keep you intact while it passes.
Urge Surfing and Mindfulness: Letting the Wave Pass
Cravings have a shape. They rise, they peak, and they fall — usually in 20 to 30 minutes if you don't feed them. The mistake most people make in early recovery is treating a craving like an emergency that has to be ended. The skill is treating it like weather.
Urge surfing is exactly what it sounds like. You notice the craving without arguing with it. You locate it in your body — tightness in the chest, heat behind the eyes, a buzzing in the hands. You watch it the way you'd watch a wave from shore. You breathe. You wait. You don't have to make it go away. You just have to outlast it.
This is the core of mindfulness-based relapse prevention, which combines meditation training with traditional relapse prevention skills. A randomized trial comparing MBRP to standard aftercare found it offered real protection for people working on long-term sobriety, and a 2025 meta-analysis grouped MBRP with CBT among the most effective evidence-based interventions for relapse prevention 16, 7.
You don't need an hour of meditation to use it. Three minutes of paying attention to your breath when a craving hits is enough to remember that the urge is a sensation, not a command. The wave will pass. You don't have to.
HALT and the Five Rules: Self-Care as Relapse Prevention
Here's a question worth asking before any big decision in recovery: am I Hungry, Angry, Lonely, or Tired?
HALT looks almost too simple to take seriously. That's the point. Most relapses don't start with a craving — they start with a missed meal, a fight you didn't process, a stretch of isolation, or a week of bad sleep 2. When any of those four are running in the background, your tolerance for everything else drops, and the part of your brain that wants to use gets louder. Run the HALT check twice a day for a week and notice how often the answer is yes to at least one. That awareness alone changes your decisions.
HALT lives inside a larger framework worth keeping close — the five rules of recovery:
- change your life
- be honest
- ask for help
- practice self-care
- don't bend the rules 2
They sound like refrigerator magnets until you watch what happens when you ignore one. Skipping self-care thins your defenses. Bending one small rule ("I'll just go to the bar to see friends") makes the next bend easier.
You don't need to perform any of this. You need to feed yourself, sleep, tell the truth about how you're doing, and ask for help before you're drowning. Boring, repeated, on the days nothing is wrong. That's the work.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Connection Is a Skill, Not a Personality Trait
Calling Someone Before You Need To
Here's the part that confuses people who haven't done this work: the phone call that protects you isn't the one you make at 11 p.m. when you're shaking. It's the one you make on Sunday afternoon when you're fine.
Connection as a skill means reaching out before there's a crisis to report. You text your sponsor on a normal Tuesday. You call a friend in the program just to say hi. You show up at the meeting when nothing is wrong. The point isn't the content of the conversation. The point is keeping the line open, because a line that's only used in emergencies tends to feel too heavy to pick up when the emergency comes 1.
If reaching out feels awkward, that's normal. Make it boring. A two-sentence text counts. "Thinking of you, hope your week is good" counts. You're practicing the muscle, not auditioning for closeness.
Peer Support and Step Work, Honestly Sized
Peer support helps. It also isn't magic, and it's worth being honest about both.
A 10-year study of AA participation found that involvement — meeting attendance, step work, helping other members — was linked to better long-term outcomes, but the abstinence rate across assessments never climbed above 13% 11. Read that carefully. It doesn't mean the program doesn't work. It means peer support is one ingredient in a longer recipe, not the whole meal. People who do well long-term tend to combine peer groups with therapy, sometimes medication, and an aftercare structure that holds them when motivation dips 1.
So size it accordingly. If AA, NA, SMART Recovery, Refuge Recovery, or a faith-based group fits your life, use it. The step work, the sharing, the showing up to help someone newer than you — those have real value, and the research backs that the helping piece especially seems to matter 11.
If a particular room doesn't fit, try another room before you decide the format is wrong. And if peer support alone isn't holding you, that's information — not a personal failure. It means you need more layers: a therapist, an outpatient touchpoint, a check-in with a prescriber. Connection isn't a single relationship. It's a small network that catches you from different angles.
Repairing the Lifestyle That Fed the Addiction
Marlatt's relapse prevention model has three pillars, and people pay attention to two of them. Skills training, cognitive restructuring — those get the airtime. The third pillar is lifestyle balance, and it's the one that quietly determines whether the first two hold 3.
Here's what that means in plain terms. The life that included using had a shape. Certain people, certain places, certain hours of the day, certain ways of handling money or boredom or Sunday afternoons. If you keep most of that shape and just remove the substance, you've built a recovery on a structure that's still tilted toward where you came from. The substance was filling a slot. If you don't refill the slot, something else will.
Lifestyle repair is the unglamorous work of redesigning the slot. What time do you wake up now? Who do you eat dinner with? What do you do at 9 p.m. on a Friday when the old version of you would have been at the bar? Where does your money go that used to go to using? What's on the calendar that you actually look forward to?
Some of this is subtraction — the relationships that only worked when you were using, the routes home that pass the liquor store, the group chat that revolves around drinking. Some of it is addition — a standing walk with a friend, a class that meets every Tuesday, a hobby that uses your hands, a job that respects your sleep. The five rules of recovery name this directly: change your life 2. Not your willpower. Your life.
Go slowly. You don't have to overhaul everything by next month. Pick one slot — one evening, one relationship, one habit — and rebuild that. Then the next. The point isn't a perfect life. It's a life that doesn't keep handing you the same setup.
Medication as Skill Support, Not a Shortcut
If you're on buprenorphine, methadone, naltrexone, or acamprosate, you've probably already heard a version of the bad take: that's not real recovery. It is. Let's be plain about that.
Medication-assisted treatment doesn't replace the skills work in this article. It makes the skills work possible. When the neurochemical pull is dialed down to a manageable volume, you have the bandwidth to actually use cognitive restructuring, run a HALT check, surf an urge, or pick up the phone. Without that bandwidth, willpower is doing all the lifting — and willpower runs out.
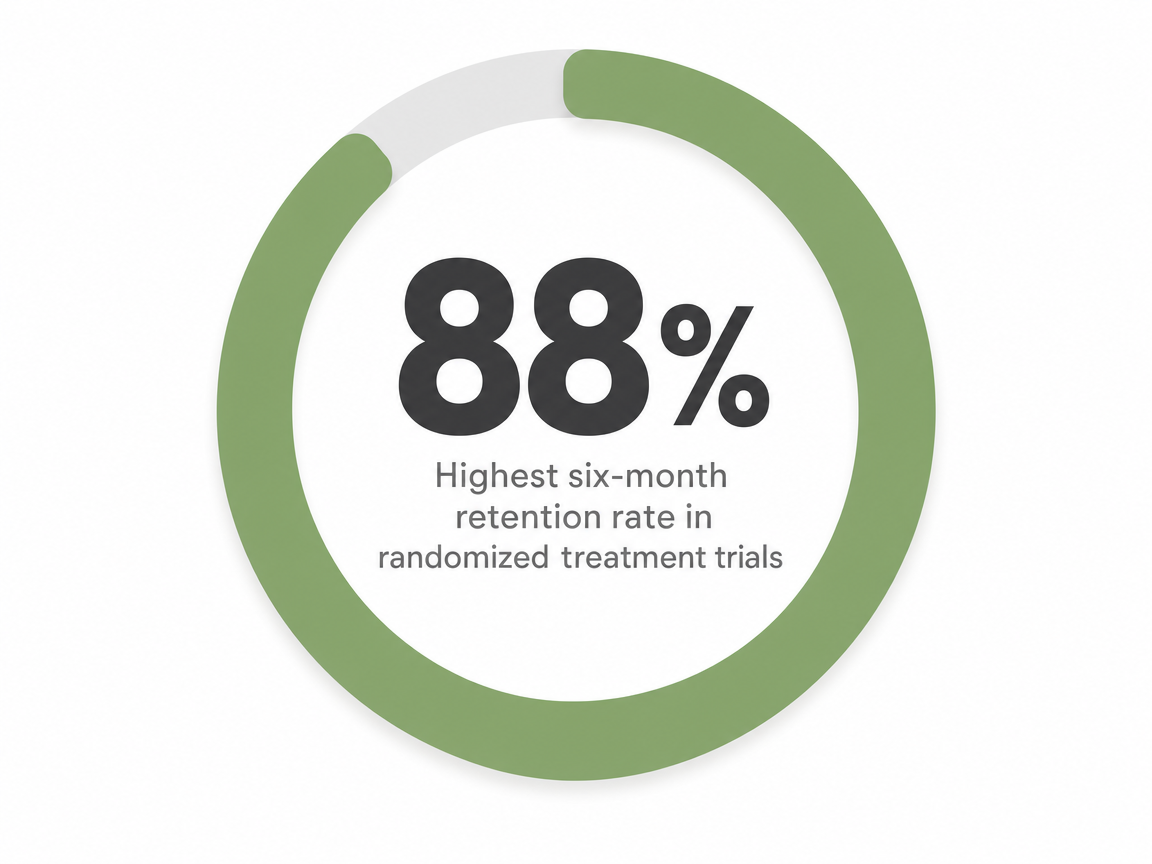
For opioid use disorder, three medications carry FDA approval and form the backbone of long-term outpatient care: methadone, buprenorphine, and naltrexone 10. The honest part of the data is that retention varies widely — six-month retention across randomized trials has ranged from roughly 3% to 88%, depending on dose, setting, and the support wrapped around it 6. That spread isn't a reason to skip medication. It's a reason to pair it with structure: regular prescriber visits, therapy, and the kind of aftercare that notices when you start drifting.
Take it on schedule. Tell your prescriber the truth. Treat the medication the way you treat the meeting — as part of the practice, not a sign that you haven't graduated.
Aftercare Is How You Keep the Skills Sharp
Skills get rusty without a place to use them. Aftercare is that place.
The structure can take a lot of shapes — a standing therapy appointment, an alumni group that meets every other Thursday, a sober living house, a continuing outpatient track that steps you down gradually instead of dropping you off a cliff. What matters isn't the format. What matters is that something on your calendar keeps asking you the questions you'd otherwise stop asking yourself: How are you sleeping? Who did you call this week? What set you off on Saturday?
Translation for your week: don't graduate yourself early. If you're in an IOP, finish it. If you're stepping down to a standard outpatient track or alumni programming, keep the appointment even on weeks you feel fine — especially on weeks you feel fine, because that's when the drift starts. Aftercare isn't remediation. It's the practice room where the scales stay sharp.
When a Hard Week Happens: Recurrence Is Data, Not a Verdict
Let's talk about the part nobody wants to say out loud.
Sometimes, despite the meetings and the meds and the meal plans, you use again. A slip. A full return. A weekend that got away from you. If that's where you are right now, or where you've been, the language matters: clinicians have moved away from relapse as a verdict and toward recurrence as what it actually is — a return of a chronic condition that needs a treatment adjustment, not a character review 12, 9.
That reframe isn't softness. It's accuracy. The skills you've been building didn't disappear. Something in the system around them — sleep, connection, structure, medication, an unprocessed grief — gave way, and the recurrence is the signal pointing at it. Treat it that way. What changed in the two weeks before? What did you stop doing? Who did you stop calling? Where did the drift start?
The action is straightforward, even when you feel ashamed. Tell someone within 24 hours — a sponsor, a therapist, a prescriber. Get back to a meeting, even the next one. Re-engage your outpatient team and let them adjust the level of care if that's what the moment calls for 9. Recurrence is hard. It is not the end of your recovery. It's the part where you find out what your skills look like when you actually need them.
Frequently Asked Questions
What are the most important recovery skills to practice in early sobriety?
Start with four: cognitive restructuring (catching the thought before you act on it), distress tolerance (riding out a hard moment without making it worse), HALT self-checks (hungry, angry, lonely, tired), and reaching out to one person before you need to. These pull from the strongest evidence base for substance use treatment and cover most situations early recovery will hand you 8, 2.
How do I know if I'm in emotional relapse before it becomes physical?
Watch the quiet signs, not the dramatic ones. Skipping meetings while still attending some, eating poorly, sleeping badly, suppressing feelings, isolating from people who know you — these stack into emotional relapse before any thought of using shows up 2. If three or more are running this week, treat it seriously. The intervention is small: eat, sleep, call someone, show up 1.
Is urge surfing actually effective, or is it just a buzzword?
It's evidence-backed. Urge surfing is the core skill of mindfulness-based relapse prevention, and a 2025 meta-analysis grouped MBRP with CBT among the most effective interventions for preventing relapse in substance use disorders 7, 16. The mechanism is simple: cravings rise and fall as sensations, not commands. You notice, breathe, and outlast. It works because you're practicing it, not because the name is clever.
Does taking medication like buprenorphine or naltrexone mean I'm not really sober?
No. Methadone, buprenorphine, and naltrexone are FDA-approved treatments for opioid use disorder and a recognized backbone of long-term outpatient recovery 10. Medication lowers the neurochemical pull so your skills work has room to land. Six-month retention in trials varies widely — roughly 3% to 88%, depending on dose and the support around it — which means medication paired with therapy and aftercare holds best 6.
How long should I stay in aftercare or a sober living environment?
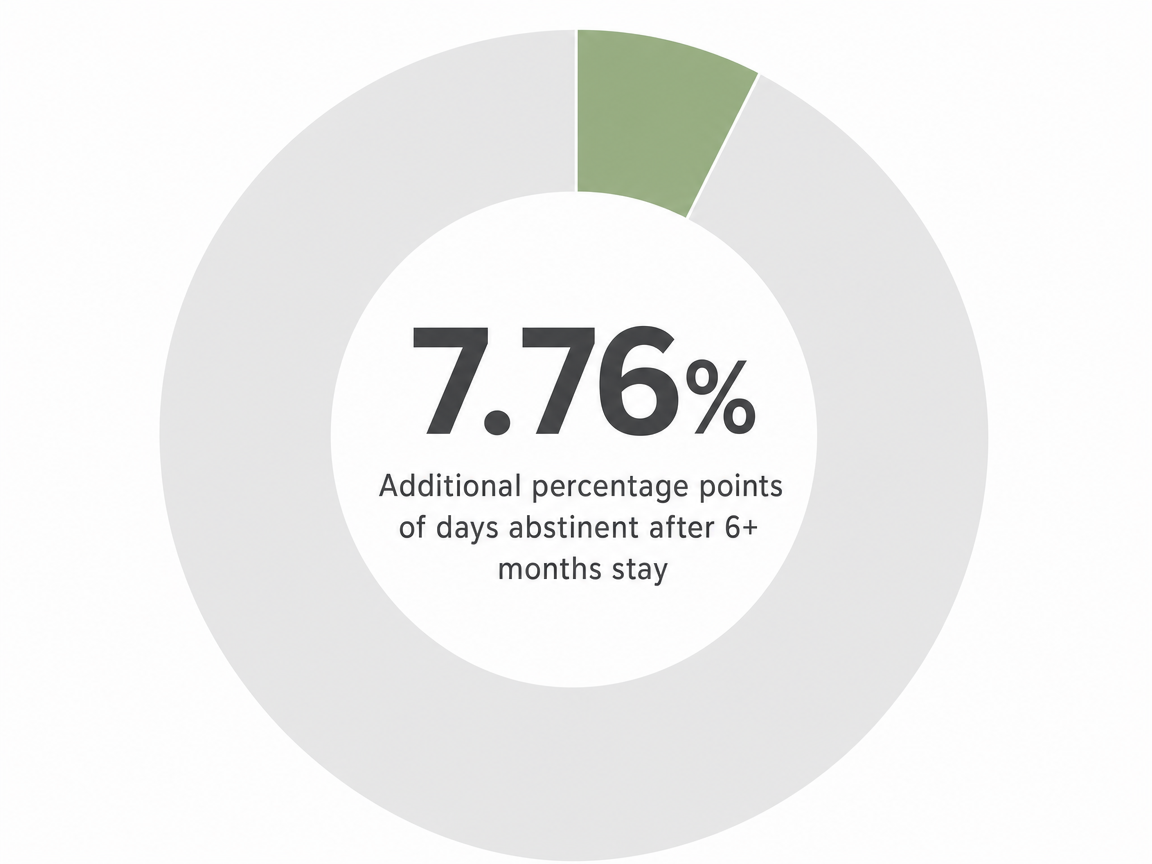
Longer than feels necessary. A 2023 study of sober living residents found that those who stayed 6 months or more reported 7.76 percentage points more days abstinent than people who left earlier 14. The same logic applies to outpatient touchpoints, alumni groups, and standing therapy — keep showing up after you feel fine. That's when the drift starts, and that's when the structure earns its keep.
What should I do if I have a recurrence after months of sobriety?
Tell someone within 24 hours — sponsor, therapist, or prescriber — and get back to a meeting, even the next one. Clinicians now frame this as recurrence of a chronic condition, not a moral verdict, and the right response is a treatment adjustment 12, 9. Look at what shifted in the two weeks before: sleep, connection, medication adherence, structure. Re-engage your outpatient team and let them recalibrate.
References
- Addiction Relapse Prevention - StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK551500/
- Relapse Prevention and the Five Rules of Recovery - PMC - NIH. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553654/
- Relapse Prevention: An Overview of Marlatt's Cognitive-Behavioral Model - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6760427/
- Relapse prevention - PMC - NIH. https://pmc.ncbi.nlm.nih.gov/articles/PMC5844157/
- Does an adapted Dialectical Behaviour Therapy skills training ... - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6694661/
- Retention in Medication-Assisted Treatment for Opiate Dependence - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6542472/
- A Meta-Analysis on Intervention for Relapse Prevention - PMC - NIH. https://pmc.ncbi.nlm.nih.gov/articles/PMC12028592/
- Cognitive Behavioral Interventions for Alcohol and Drug Use Disorders - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC5714654/
- Chapter 7—From Action to Maintenance: Stabilizing Change - NCBI. https://www.ncbi.nlm.nih.gov/books/NBK571075/
- Medication Assisted Treatment for Opioid Use Disorder - PMC - NIH. https://pmc.ncbi.nlm.nih.gov/articles/PMC8389722/
- The 10 Year Course of AA Participation and Long-Term Outcomes. https://pmc.ncbi.nlm.nih.gov/articles/PMC3558837/
- TIP 35: Enhancing Motivation for Change in Substance Use Disorder Treatment - SAMHSA. https://www.samhsa.gov/resource/ebp/tip-35-enhancing-motivation-change-substance-use-disorder-treatment
- Behavioral Therapies | NIDA. https://nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/evidence-based-approaches-to-drug-addiction-treatment/behavioral-therapies
- Six-month length of stay associated with better recovery outcomes ... - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12841932/
- Summary of Evidence - Inpatient and Outpatient Treatment ... - NCBI. https://www.ncbi.nlm.nih.gov/books/NBK507689/
- Relative efficacy of mindfulness-based relapse prevention ... - PubMed. https://pubmed.ncbi.nlm.nih.gov/24647726/



