
Weighing the Benefits of Intensive Outpatient Treatment

Key Takeaways
- Outcome data shows 50% to 70% of IOP participants report abstinence at follow-up, with results comparable to inpatient care for most patients who can safely engage from home 1.
- IOP typically requires 9 to 12 clinical hours across 3 to 5 days per week, with a 90-day minimum reflecting evidence that sustained engagement outperforms brief, high-intensity treatment 14.
- Integrated medication-assisted treatment paired with CBT lowers positive drug screens compared to counseling alone, making on-site coordination between prescribers and therapists a key program-quality marker 16.
What the Outcome Data Actually Says About IOP
The most crucial finding about intensive outpatient programs (IOPs) is often overlooked: studies show that between 50% and 70% of participants report abstinence at follow-up, and for most patients, these outcomes are comparable to those achieved in inpatient settings 1. This outcome parity, on the metric that truly matters, is the headline. It's not just about flexibility, convenience, or lower cost.
If you've been led to believe that effective treatment requires leaving your life behind for an extended period, it's time to re-evaluate that perspective. The evidence, drawn from randomized trials and quasi-experimental studies, indicates that continuity of care over time often outweighs the intensity of a short-term treatment burst. Sustained engagement at a manageable level frequently yields better results than a brief, high-intensity stay without ongoing support, particularly for individuals with long-standing addiction histories 1.
This doesn't imply that inpatient care is ineffective or that IOP is inherently superior. Instead, it suggests that the choice between them depends on your specific clinical needs and life circumstances. For someone who can maintain safety at home, has a stable living environment free from active substance use, and can consistently attend sessions, data indicates that an IOP can lead to the same positive outcomes as a residential program.
This offers a different kind of reassurance than typically found in articles. You don't necessarily have to abandon your job, family, or housing to receive effective treatment. However, consistent participation, week after week, for a sufficient duration is essential for the treatment to be effective. The remainder of this article will explore what "sufficient duration" entails, the typical weekly schedule, and when IOP is, and isn't, the most appropriate choice.
How IOP Fits into the Continuum of Care
It's helpful to view addiction treatment as a spectrum of care rather than a single option. The American Society of Addiction Medicine categorizes care into five levels, ranging from weekly therapy to medically managed inpatient treatment. Intensive outpatient programs occupy a middle ground: they offer more frequent contact than weekly therapy but are less intensive than partial hospitalization or residential care 14.
Medicare defines IOP as a recognized level of care for mental health conditions, including substance use disorders, positioned between traditional weekly therapy and more intensive services like partial hospitalization or inpatient treatment 10. This federal definition is significant because it confirms that IOP is a covered benefit, not merely a marketing term. It also highlights the flexibility to transition to different levels of care if your needs evolve.
This level of treatment is not designed to be permanent. A recommended minimum duration for IOP is around 90 days, as sustained engagement at a lower intensity often leads to better outcomes than short, high-intensity interventions 14. Many individuals transition to IOP after completing a residential stay or partial hospitalization to maintain progress. Others begin with IOP because it aligns with their clinical needs and later step down to standard outpatient care as their stability improves.
The key takeaway is that you can adjust your treatment level as your situation changes. If you require more support, you can escalate care. If you achieve greater independence, you can de-escalate. IOP serves as a flexible middle ground, adapting to your needs rather than being a rigid, fixed destination.
A Typical Week in an IOP
A common question about IOPs, often vaguely addressed by programs, concerns the practical aspects: how many hours, on which days, and at what times? Typically, intensive outpatient programs involve 9 to 12 clinical hours per week, spread over 3 to 5 days. Programs often offer morning, afternoon, or evening tracks to accommodate work or family responsibilities 13. This structure provides both a promise of flexibility and a demand for commitment.
A typical week might involve attending group therapy three evenings a week, for example, Monday, Wednesday, and Thursday from 6 to 9 p.m., with a weekly individual therapy session scheduled during a lunch break or before work. Morning tracks often run from 9 a.m. to noon, suiting certain shift workers or self-employed individuals. Afternoon tracks offer a middle-ground option. Regardless of the chosen track, the clinical content remains consistent: a blend of group therapy, individual sessions, psychoeducation, skills practice, and, for many participants, integrated medication management appointments.
The duration of treatment is as important as the weekly hours. A minimum stay of approximately 90 days in IOP is recommended, as sustained engagement at this intensity is consistently linked to better outcomes than shorter, more intense treatment periods 14. Three months represents a significant commitment, yet it's often less time than people anticipate for "treatment," and the hours are designed to integrate with your life rather than disrupt it.
Consider this practical scenario: after a demanding Tuesday at work, you grab dinner in your car and arrive at a 6 p.m. group session still wearing your work ID. Initially, this might feel unusual. By week six, it becomes a routine Tuesday. You might discuss a workplace interaction from that morning where an old urge resurfaced, and the group helps you process it before it escalates. That same evening, you return home, sleep in your own bed, and wake up to your usual family and alarm. The treatment doesn't pause your life; it becomes an integrated part of it.
If your schedule is exceptionally rigid, it's crucial to communicate this during your intake assessment. A reputable program will work with you to find a suitable track or provide referrals if a fit isn't possible. Consistent attendance for 90 days is the core of the work; the rest is logistical.
Clinical Benefits and Mechanisms of IOP
Practicing Skills Against Real Triggers
One unique advantage of IOP that residential treatment cannot fully replicate is the opportunity to manage real-life triggers in your actual environment. This means addressing challenges like an argument with a partner on a Thursday night, a coworker who still drinks at lunch, or the familiar route home that passes an old liquor store. These aren't simulated scenarios; they are real-time experiences that you bring to your group sessions for processing.
This immediate feedback loop contributes to why longer, sustainable engagement often yields better results than short, intense treatment bursts, especially for individuals with deeply ingrained addiction patterns 1. Skills are not merely practiced in a controlled environment and then applied to the outside world. They are tested in real-life situations, with the immediate support of clinicians and a group to help debrief and strategize.
It's inevitable that you will encounter setbacks. A coping skill might not work as intended, or you might experience a craving unexpectedly. These moments are not failures of treatment; they are integral to the treatment process itself. The clinical work in IOP is designed to bring these experiences into the therapeutic setting, identify what happened, and explore alternative approaches for the future. Skills become truly effective when they are refined through real-world application, not just hypothetical exercises.
Integrated Medication-Assisted Treatment and Behavioral Therapy
For individuals dealing with opioid or alcohol use disorders, a critical clinical consideration is the combination of medication and therapy. Research consistently highlights the effectiveness of this integrated approach.
A comparative effectiveness study involving 40,885 adults with opioid use disorder examined six different treatment pathways. It found that only buprenorphine or methadone were associated with reduced overdose risk and decreased serious opioid-related acute care utilization at both 3-month and 12-month follow-up points, compared to no treatment 5. Counseling alone, residential stays without medication, and even hospital detox without a medication handoff did not demonstrate the same level of protective effect.
Therapy remains vital, and its impact is amplified when combined with medication. Another study showed that MAT patients who received integrated cognitive behavioral therapy had significantly lower odds of a positive urine drug screen compared to non-medicated patients receiving standard counseling alone 16. These two interventions complement each other: medication stabilizes the brain chemistry that can make early recovery feel overwhelming, while therapy provides the tools to build a fulfilling life that medication makes possible.
SAMHSA's comprehensive review of MAT outcomes further illustrates its benefits, including improved survival rates, longer treatment retention, reduced illicit opioid use, better employment outcomes, and improved birth outcomes for pregnant women in recovery 3. These are not minor benefits; they are fundamental to achieving lasting recovery.
In an IOP setting, this integration is highly practical. You avoid the complexity of managing medication with one provider and therapy with another, hoping they communicate. A program structured around integrated care places the prescriber, therapist, and group facilitator in the same location, often on the same day, working from a shared record. If something changes in your week, the entire team is aware and can respond collaboratively. This integrated approach is a key mechanism of IOP's effectiveness and why it's one of the few settings where such comprehensive care can be delivered efficiently within the rhythm of your daily life.
Trauma-Informed Pacing and Dual Diagnosis
For many individuals, substance use is intertwined with underlying issues such as past trauma, untreated anxiety, depression, or unresolved experiences that impact their well-being. A treatment approach that addresses only substance use while neglecting these co-occurring conditions is only tackling half the problem.
Trauma-informed care is a fundamental clinical framework that recognizes how traumatic stress reactions influence engagement in treatment, interactions with staff, and overall outcomes 9. Clinicians trained in this approach interpret behaviors like a flat affect or a missed session differently. They don't view it as resistance but as valuable information about an individual's nervous system, allowing them to tailor the pace of treatment accordingly.
This pacing is crucial. In a competent IOP, you won't be pressured to disclose trauma prematurely just because a curriculum dictates it. Instead, you'll be offered choices, predictable structure, and sufficient time to feel safe enough to address more challenging material when you are ready. For working adults already navigating life's demands, this thoughtful pacing can be the difference between staying in treatment and quietly disengaging. Dual diagnosis care, integrated from the initial intake, treats conditions like depression, PTSD, or anxiety as interconnected parts of the same overall challenge, rather than separate issues to be addressed sequentially.
Practical DBT and CBT Skills
The primary therapeutic modalities encountered in IOP are cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT), both designed for practical application.
CBT helps you identify the connection between your thoughts, feelings, and behaviors, providing strategies to interrupt unhelpful patterns before they lead to substance use. For example, if the thought is "I can't get through this meeting sober," leading to dread, and the old behavior was drinking at 11 a.m., CBT teaches you to challenge that thought, assess its validity, and choose a different response.
DBT was developed for individuals who experience intense and rapidly shifting emotions, a common experience in early recovery. This treatment encompasses five core functions: enhancing motivation for change, developing new skills, facilitating the generalization of new behaviors into daily life, structuring the environment to support change, and providing support for the therapist 12. In an outpatient setting, these functions are delivered through individual therapy, group skills training, phone coaching between sessions, and a consultation team 12. DBT-informed approaches in partial hospital and IOP settings are particularly effective for addressing emotion dysregulation, self-harm, and substance use concurrently, which is a common presentation for many individuals seeking treatment 7. You will acquire tangible skills that you can apply in real-time situations, rather than just theoretical concepts.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Determining if IOP is the Right Fit
It's important to acknowledge an honest trade-off often not explicitly stated: inpatient participants are approximately three times more likely to complete treatment than outpatients 15. While this gap doesn't mean inpatient outcomes are three times better, and overall evidence still shows comparable abstinence rates for most individuals 1, completion is a significant metric. When considering IOP, you deserve to see this data rather than have it obscured.
IOP is generally suitable when several conditions are met. You should be medically stable, without risk of severe withdrawal requiring 24-hour monitoring. Your living environment needs to be reasonably safe, meaning household members are not actively using substances, and there is no ongoing violence. You must be able to maintain sufficient consistency—with a job, transportation, and communication—to attend sessions three to five days a week for approximately 90 days 14. Additionally, any co-occurring mental health conditions should be stable enough to be addressed concurrently with substance use, rather than requiring prior stabilization 9. This applies across opioid, alcohol, and stimulant use disorders, including populations addressed by the 2024 ASAM/AAAP guideline for stimulant use 6.
The good news is that this is not a one-time decision. Many individuals begin in residential or partial hospitalization programs, stabilize, and then transition to IOP to maintain momentum as they reintegrate into their lives. A comprehensive intake assessment, which explores your withdrawal history, living situation, psychiatric history, and past treatment challenges, is crucial for you and a clinician to determine the most suitable starting point. If a program attempts to admit you without such a thorough conversation, it provides important information about that program's approach.
The Rationale Behind IOP's Existence
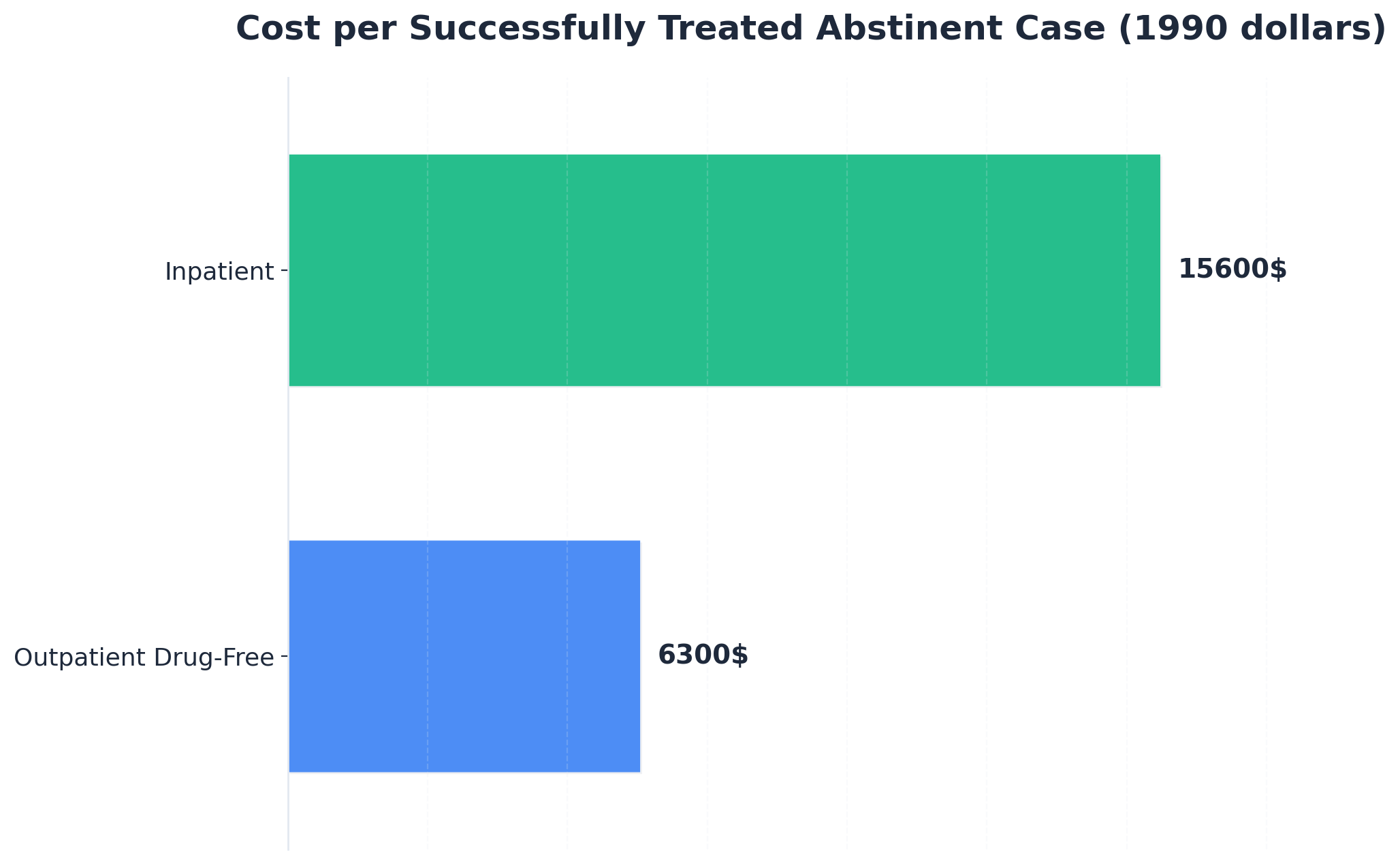
IOP did not emerge as a cheaper alternative to traditional rehab. Its development was driven by honest cost-effectiveness data in substance use treatment, which revealed a specific pattern: while differences in effectiveness across modalities were often small, the differences in cost per successful outcome were substantial. The Drug Abuse Treatment Outcome Studies, for instance, found that the cost per successfully treated abstinent case was approximately $6,300 in outpatient drug-free programs compared to about $15,600 in inpatient programs, in 1990 dollars 8. Although these figures are dated and absolute values would change with inflation, the consistent ratio between settings significantly influenced policy.
This cost-effectiveness ratio is a primary reason why Medicare and most commercial insurers integrated IOP into the covered continuum of care, positioning it between weekly therapy and partial hospitalization 10. Payers were not acting out of charity; they were responding to evidence indicating that for most patients, comparable abstinence outcomes could be achieved at a lower cost if the program structure was appropriate and the duration sufficient. The 90-day minimum is also not arbitrary; it reflects research demonstrating that longer engagement at a sustainable intensity consistently leads to better outcomes than short, expensive bursts of care 14.
For you, this means IOP is not merely a budget option to settle for. It represents a level of care developed by the system after seriously considering both outcome and cost data. Coverage exists, and the clinical justification is strong. The more critical question becomes identifying a program that effectively utilizes those 90 days.
What Completers Report About IOP
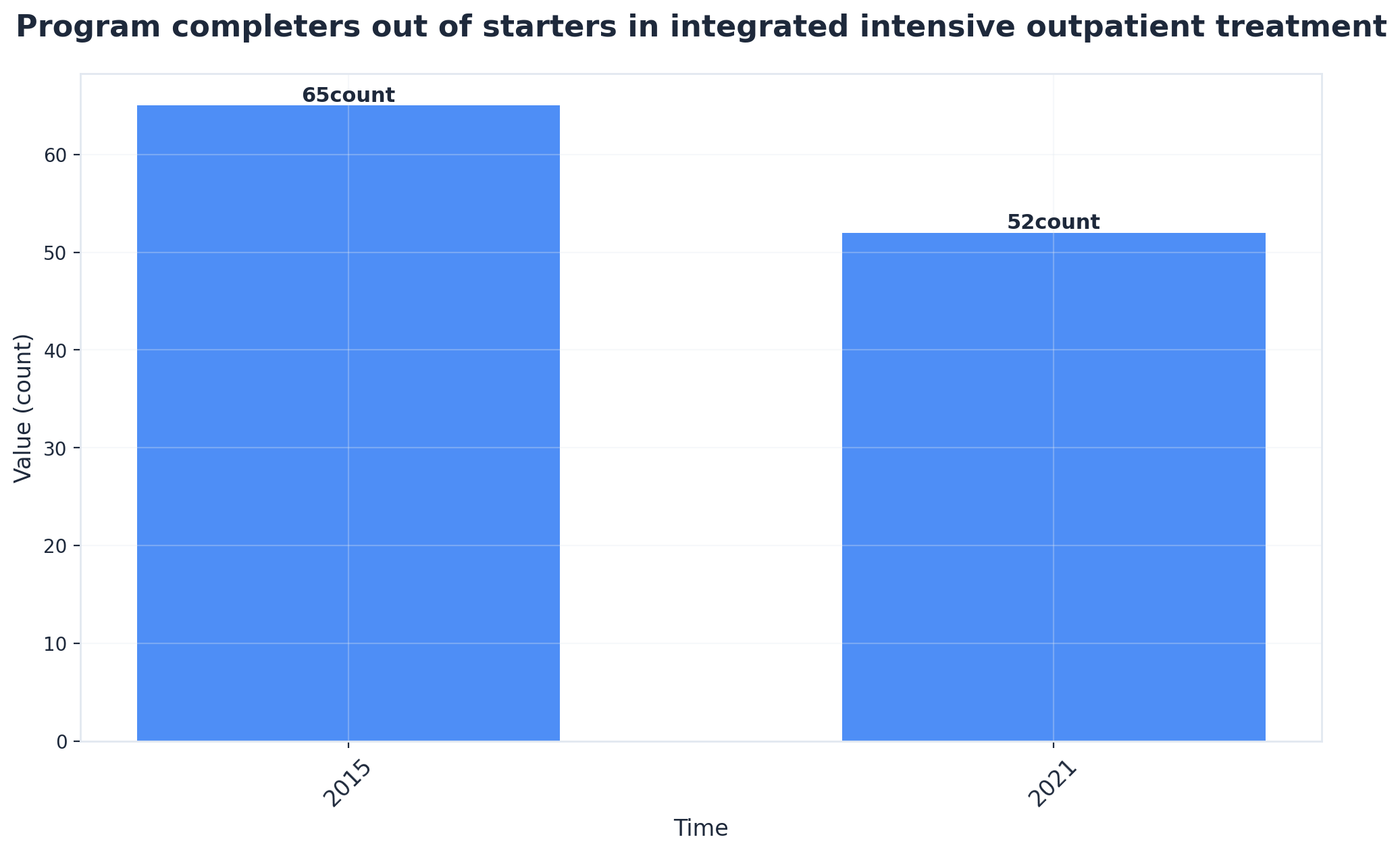
It's valuable to understand the experiences of individuals who have successfully completed IOP. A 2025 qualitative study of adults who finished a four-month integrated intensive outpatient program reported high satisfaction among completers, strong working relationships with clinical staff, and tangible self-development gains they could articulate 2. They didn't describe a miraculous cure but rather a sense of being understood by their treatment team and observing how their group work influenced their decisions at home.
The therapeutic alliance is more significant than it might initially seem. When you engage with a clinician who consistently tracks your progress over weeks and notices subtle shifts, treatment transcends a mere checklist and evolves into a meaningful relationship. This relational aspect is what completers often emphasize—not just the curriculum or homework, but the supportive environment, the people, and the experience of being held accountable while being treated as a capable adult with a life worth reclaiming.
Choosing an Effective IOP
Once you've determined that IOP is the appropriate level of care, the next step is selecting a program. Ninety days is a significant portion of your life, and not all programs will utilize that time effectively.
Before committing, consider asking several key questions. Inquire whether the intake process includes a comprehensive assessment of your withdrawal history, psychiatric history, living situation, and any previous unsuccessful treatments. If a program is willing to admit you without such a thorough conversation, it may indicate how the subsequent 90 days will unfold. Ask if medication-assisted treatment (MAT) is offered on-site and coordinated directly with your therapy team, rather than requiring referrals to an external prescriber. The research on integrated MAT and behavioral care is clear 16, and a program that externalizes medication management may be overlooking evidence-based practices.
Also, ask how trauma is addressed within the curriculum. A program that allows for paced disclosure and offers choices about what to work on, and when, aligns with research-supported frameworks 9. Inquire about scheduling options: morning, afternoon, and evening tracks should be genuinely available, not just theoretical possibilities. Finally, ask about the process for stepping up or stepping down a level of care if your needs change during treatment.
If you are in South Portland or the surrounding area, Coastal Recovery Partners is an example of a program where these integrated elements are foundational to the design. Regardless of where you seek treatment, the right program will prioritize your entire well-being, not just the aspects that are easily billable.

Frequently Asked Questions
How many hours per week does intensive outpatient treatment require?
Most IOPs typically involve 9 to 12 clinical hours per week, spread across 3 to 5 days. Programs often offer morning, afternoon, or evening tracks to accommodate work or caregiving schedules 13. It's advisable to plan for a minimum stay of 90 days, as longer engagement at this intensity is consistently associated with better outcomes 14.
Is IOP as effective as inpatient rehab?
For the majority of patients, yes. Evidence syntheses on IOP effectiveness indicate that 50% to 70% of participants report abstinence at follow-up, with outcomes that are not significantly different from those achieved in inpatient settings 1. However, it's important to note that inpatient participants are approximately three times more likely to complete treatment than outpatients 15, highlighting the importance of consistent attendance in IOP.
Can I keep working or caring for my family while in IOP?
Yes, this is a core design principle of IOP. Schedules are structured with morning, afternoon, and evening tracks specifically to allow you to maintain employment, care for your children, and sleep at home while engaging in clinical work 13. The challenge lies in consistently prioritizing these treatment hours, much like you would a medical appointment, as three to five sessions per week for 90 days requires significant commitment.
Does IOP include medication-assisted treatment for opioid or alcohol use disorder?
A well-designed IOP integrates medication-assisted treatment (MAT) with therapy directly on-site, rather than referring it out. Research clearly demonstrates that MAT patients who receive integrated cognitive behavioral therapy have significantly reduced odds of a positive urine drug screen compared to non-medicated individuals receiving standard counseling 16. Furthermore, MAT broadly improves survival, treatment retention, employment outcomes, and birth outcomes 3. When considering programs, ask if the prescriber and therapist collaborate using a shared patient record.
When is IOP not the right level of care?
IOP is not the appropriate starting point if you are at risk of severe alcohol or benzodiazepine withdrawal requiring medical monitoring, if you are experiencing an active suicidal crisis, or if your home environment is not safe enough to support recovery. A trauma-informed assessment of your nervous system, living situation, and psychiatric history is essential for a clinician to determine if partial hospitalization or residential care is needed first 9. These considerations are about finding the most effective level of support for your current needs.
Does insurance or Medicare cover intensive outpatient treatment?
Yes. Medicare explicitly covers IOP as a recognized level of care for mental health conditions, including substance use disorders, positioning it between weekly therapy and partial hospitalization 10. Most commercial insurers follow a similar continuum-of-care framework. The intake or care coordination team at a program can verify your specific benefits before you commit to the 90-day program.
References
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Clients' Experiences and Satisfaction with an Integrated Intensive Outpatient Program. https://pmc.ncbi.nlm.nih.gov/articles/PMC11898248/
- Treatment Options for Substance Use Disorder - SAMHSA. https://www.samhsa.gov/substance-use/treatment/options
- An Overview of Medication-Assisted Treatment for Opioid Use Disorders. https://icjia.illinois.gov/researchhub/articles/an-overview-of-medication-assisted-treatment-for-opioid-use-disorders-for-crimin
- Medication-Assisted Treatment for Opioid Use Disorder in a Rural Family Medicine Practice. https://pmc.ncbi.nlm.nih.gov/articles/PMC7278292/
- The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC11105801/
- DBT-Informed Treatment in a Partial Hospital and Intensive Outpatient Setting. https://pmc.ncbi.nlm.nih.gov/articles/PMC7513610/
- Effectiveness and Cost-Effectiveness of Four Treatment Modalities for Substance Disorders at DATOS Sites. https://pmc.ncbi.nlm.nih.gov/articles/PMC1360883/
- Understanding the Impact of Trauma. https://www.ncbi.nlm.nih.gov/books/NBK207191/
- Mental Health Care (Intensive Outpatient Program Services) - Medicare. https://www.medicare.gov/coverage/mental-health-care-intensive-outpatient-program-services
- Substance Use Disorders - Statutes, Regulations, and Guidelines. https://www.samhsa.gov/substance-use/treatment/statutes-regulations-guidelines
- Dialectical Behavior Therapy for Substance Abusers. https://pmc.ncbi.nlm.nih.gov/articles/PMC2797106/
- TIP 47: Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. https://www.samhsa.gov/resource/ebp/tip-47-substance-abuse-clinical-issues-intensive-outpatient-treatment
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Summary of Evidence - Inpatient and Outpatient Treatment for Substance Use Disorders. https://www.ncbi.nlm.nih.gov/books/NBK507689/
- The Impact of Addiction Medications on Treatment Outcomes for Opioid Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC4866634/
- Medication Assisted Treatment Program Policies: Opinions of Patients and Providers. https://pmc.ncbi.nlm.nih.gov/articles/PMC10467182/



