
How to Choose Dual Diagnosis Treatment Centers Near Me

Key Takeaways
- If past treatment didn't hold, the structure may have failed you — programs built for one condition often leave the other untreated, and that's worth questioning before blaming yourself.
- Three care models exist: sequential, parallel, and integrated. Only integrated treatment puts one team on one plan addressing both conditions together, which research supports as the standard 6.
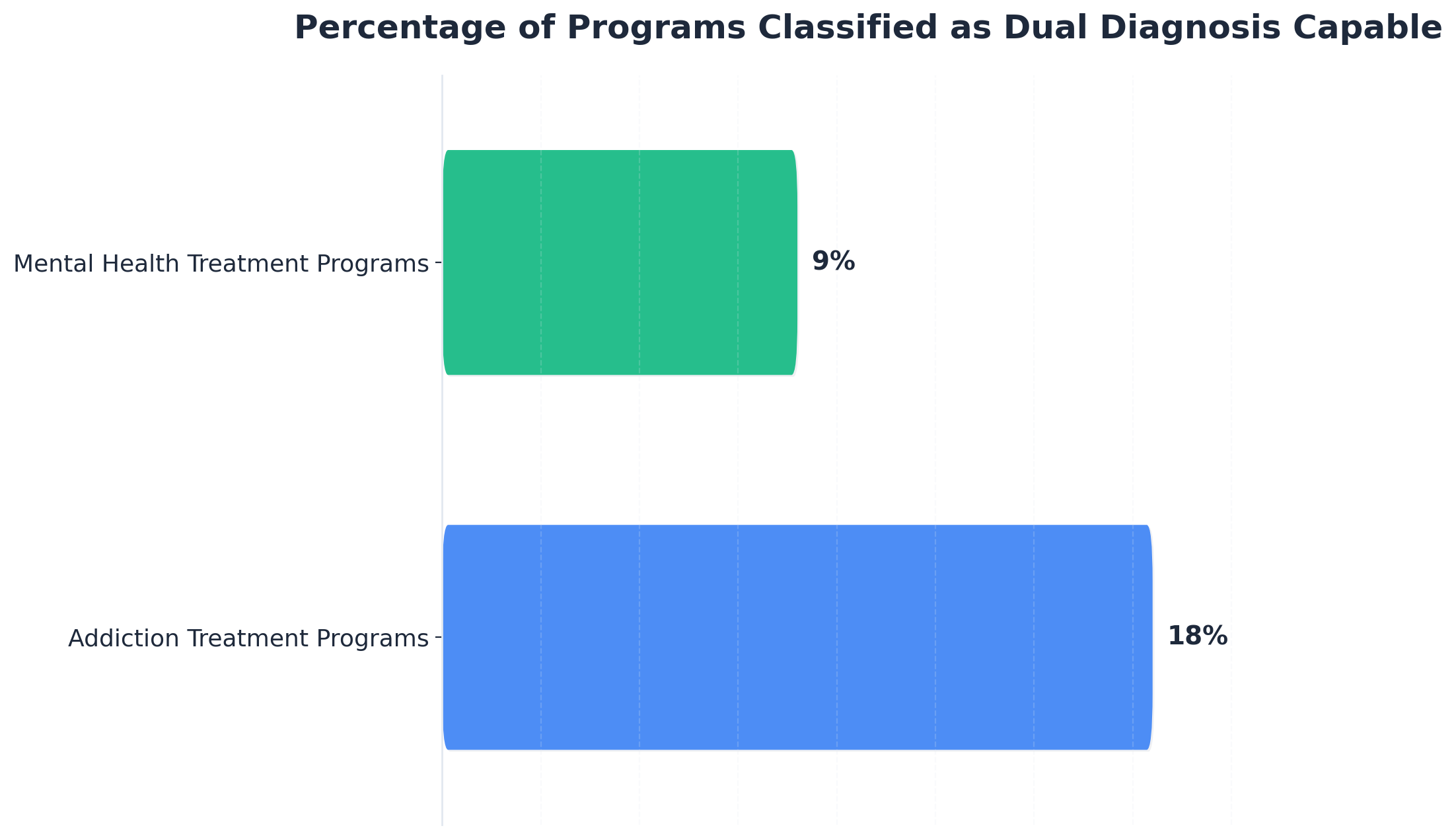
- Dual diagnosis capability is rarer than marketing suggests — only about 18% of addiction programs and 9% of mental health programs hit the capable threshold, so the label on the door means little 1.
- Clinicians use DDCAT, IDDT, and ASAM to grade programs. Knowing these tools lets you ask sharper questions and read a program's answers honestly instead of taking brochures at face value.
- A real intake screens for both substance use and mental health on the first call, names specific assessment tools, and describes a team that meets together about your plan 5.
- In Maine, verify licensing through DHHS Division of Licensing and Certification — programs may hold a mental health license, a substance use license, or both, and that distinction defines real capacity 2.
- Residential isn't always required. ASAM Criteria matches you to outpatient, IOP, PHP, or residential based on withdrawal risk, stability, and home environment, so placement fits your actual life 10.
- Ask directly about insurance coverage, weekly costs, scheduling around work or caregiving, and care coordination — practical logistics often determine whether treatment actually starts and continues.
Why your last treatment may not have failed you
If you've been through treatment before and ended up back where you started, you may be carrying a quiet belief that you're the problem. You're not.
Here's what often actually happened: you walked into a program built to treat one half of what you're living with. Maybe the rehab focused hard on the drinking but treated the panic attacks as something to deal with later. Maybe the therapist was excellent on the depression but flinched a little every time substances came up. You were asked to split yourself in two and hand each half to a different team that didn't really talk to each other.
That's called parallel treatment, and it's one of three models you'll run into when you start searching. The research is clear that integrated care — one team, one plan, both conditions treated together — produces better outcomes than addiction services and mental health services running on separate tracks 67. People with co-occurring disorders also face a higher risk of hospitalization than people with only one condition, which makes the cost of fragmented care more than just inconvenient 7.
So if a previous episode didn't hold, it's worth asking a different question this time. Not what's wrong with me, but was that program actually built to treat both things at once?
That shift — from blaming yourself to evaluating the system — is the real first step. And the fact that you're reading this means you've already taken it.
Sequential, parallel, or integrated: the three models you'll actually encounter
Once you start calling around, you'll find that almost every program says it treats co-occurring disorders. The brochures sound similar. The websites use the same phrases. The difference shows up in how care is actually structured behind the scenes — and that structure falls into three distinct models 6.
Sequential treatment means you handle one condition first, then the other. Detox and addiction treatment now, depression treatment later. Or stabilize the bipolar disorder first, then come back for the substance use piece in six months. On paper it sounds orderly. In practice, the untreated condition keeps pulling at the one being treated, and most people don't make it cleanly to phase two.
Parallel treatment is what trips up the most people. You're getting both kinds of care at the same time — but from two different teams, in two different buildings, with two different treatment plans. Your therapist down the street is working on trauma. Your addiction counselor across town is working on relapse prevention. Nobody is sitting in the same room comparing notes. When the trauma work stirs something up on a Tuesday and you drink on Wednesday, neither team sees the full picture. Parallel care can look comprehensive from the outside while quietly leaving the handoffs broken 6.
Integrated treatment is the model the research supports as the standard of care. One clinical team. One treatment plan. Both diagnoses addressed in the same sessions, by clinicians trained to hold both at once. As the federal treatment guidance puts it plainly, integrated care “addresses all of a client's diagnoses and symptoms within one service system” 6. That's not a marketing line. It's a structural commitment that changes what happens on a Tuesday afternoon when you walk through the door.
Here's a simple test. Ask a program: If my anxiety spikes mid-treatment, who adjusts my care plan, and how fast? In a sequential model, you wait. In a parallel model, you call the other provider and hope the message lands. In an integrated model, the same team that's treating your substance use can shift your therapy approach in the next session, coordinate with the prescriber down the hall, and update one plan that everyone is reading from.
You don't need to memorize these labels. You just need to know they exist, because once you can name the model, you can hear which one a program is actually offering — no matter what word they use on the homepage.
The capability gap: why integrated programs are harder to find than they should be
Here's something worth knowing before you start dialing: even though almost every brochure claims to handle co-occurring disorders, the actual capacity to do it is far rarer than the language suggests. When researchers used the DDCAT toolkit to assess addiction programs and the parallel DDCMHT tool to assess mental health programs, only about 18% of addiction treatment programs and roughly 9% of mental health treatment programs scored at the “Dual Diagnosis Capable” threshold or higher 1. The rest were technically allowed to serve people with both conditions, but didn't have the structure, staffing, or assessment process to do it well.
That gap isn't your imagination. It's why your last search may have felt confusing — the marketing language across programs is nearly identical, even when the underlying capability is wildly different.
It's also why this search takes more than a Google ranking. A program at the top of a local map result can still be an “addiction-only” program with a counselor who happens to have some mental health training. Another program with a quieter web presence may have been quietly building integrated capacity for years. The label on the door tells you very little.
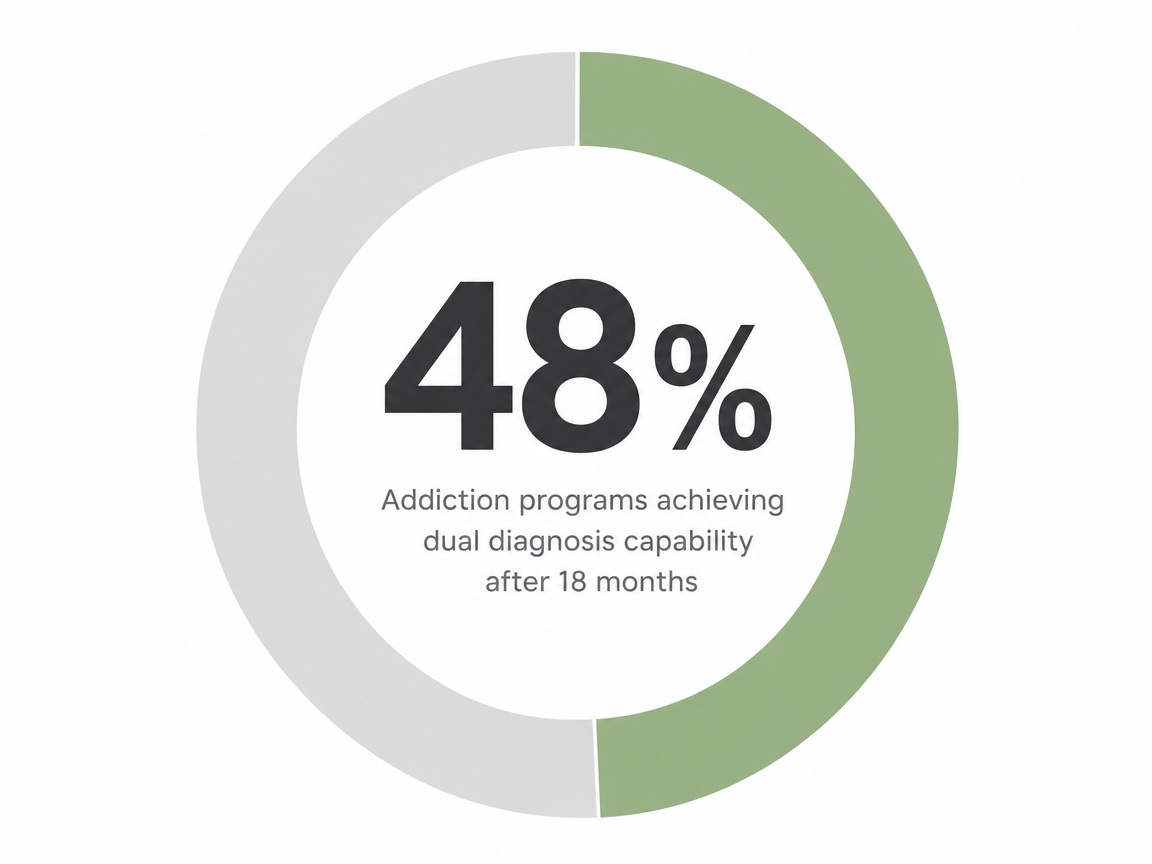
The good news: capacity isn't fixed. Programs that commit to the work can move significantly — one study tracked addiction programs that climbed from 11% to 48% dual diagnosis capable over 18 months once they started measuring themselves against a real standard 13. So when you call a program, it's fair to ask not just are you dual diagnosis capable, but how are you tracking and improving that capability. The programs doing the work will have an answer ready.
How clinicians grade a program — and how you can borrow their tools
You don't need a clinical degree to evaluate a program. You just need to know that clinicians already have standardized tools for this exact job — and the questions those tools ask are questions you can ask too.
Three names come up again and again in the research: DDCAT, IDDT, and ASAM. They sound like alphabet soup the first time you meet them, but each one answers a different question you actually care about. DDCAT (and its mental-health counterpart DDCMHT) tells you how capable a program is at handling both conditions. The IDDT Fidelity Scale tells you how faithfully a program follows the integrated treatment model. ASAM Criteria tells you what level of care — outpatient, intensive outpatient, partial hospitalization, residential — actually fits your situation.
You won't be administering these tools. But once you know they exist, the program's answers to your questions land differently. A program that can talk fluently about its DDCAT score, its fidelity to IDDT, or how it uses ASAM Criteria for placement is showing you something. A program that goes quiet, changes the subject, or says “we just do good work” is also showing you something. Both signals are useful.
The next two pieces walk through what each tool measures and how to translate it into a phone call.
DDCAT and DDCMHT: the 1–5 scale that tells you what a program can actually handle
DDCAT stands for Dual Diagnosis Capability in Addiction Treatment. DDCMHT is the same idea applied to mental health programs. Researchers built both tools to score programs on a 1–5 scale across domains like program structure, assessment process, treatment planning, staff training, and continuity of care 9.
Here's the scale, plain and simple. Programs scoring 1 to 1.99 are single-focus — addiction only or mental health only, with little real capacity for the other condition. Programs in the 2 to 2.99 range are intermediate, meaning they're aware of co-occurring disorders but haven't fully built the structure to treat them. A score of 3 or higher is the threshold for “Dual Diagnosis Capable” — the program can genuinely treat both conditions in one place. Scores of 4 and above reach “Dual Diagnosis Enhanced,” the strongest tier, where dual diagnosis isn't a side capability but the core of how the program is designed 9.
You can borrow this directly. On a call, ask: Has your program ever been assessed using DDCAT or DDCMHT? What was the score, and which domains came back strongest? You're listening for specifics — assessment processes, integrated treatment plans, prescriber access, staff with cross-training in both addiction and mental health. If the answer is a vague “yes, we treat both,” that's a 1 or 2 in disguise. If the answer names actual domains the program has worked on, you're closer to the threshold that matters.
IDDT fidelity and ASAM placement: the other two names worth knowing
The IDDT Fidelity Scale measures how closely a program actually follows the Integrated Dual Disorder Treatment model in daily practice 4. DDCAT asks whether a program can do integrated care. IDDT fidelity asks whether the program does it — in the room, in the treatment plan, in the way clinicians coordinate.
ASAM Criteria is different. It's the most widely used framework in the country for matching a person to the right level of care — outpatient, intensive outpatient, partial hospitalization, residential — and for deciding when to step up or step down 10. A program that uses ASAM Criteria isn't guessing where you belong. It's running a structured assessment.
Ask: Do you assess placement using ASAM Criteria, and does your team have training in IDDT? A clear yes tells you the program is operating inside the same standards clinicians use everywhere else.
What a real intake screening sounds like
The first phone call tells you more than the website does. Pay close attention to what they ask you.
A program built for co-occurring disorders will screen for both conditions at intake, every time, no exceptions. The federal guidance is direct on this point: substance use providers should screen all new clients for co-occurring mental disorders, and mental health providers should screen for any substance misuse 5. That means within the first conversation — not weeks into treatment — someone should be asking about your drinking and your drug use, your mood, your sleep, your trauma history, your medications, and how those pieces interact.
If the intake call only asks what you're using and how often, that's a flag. If it only asks about depression and anxiety and skips the substance questions, that's the same flag from the other direction.
Listen for what comes next. A capable program will mention specific tools or assessments — not just “our counselor will meet with you.” They might reference structured screeners, an ASAM-based placement assessment, or a psychiatric evaluation built into the first week 10. They should be able to tell you who reviews the results, how the treatment plan gets written, and whether one team owns both diagnoses or hands part of it off.
Ask outright: Who will be on my treatment team, and do they meet together about my care? The answer should name roles — therapist, prescriber, case manager — and describe a regular team meeting where your plan is actually discussed. Vague reassurance is not the same as a structure.
Maine licensing in one place: what a South Portland search should verify
Before you hand over your insurance card, take five minutes to confirm a program is actually licensed to do what its website says it does. In Maine, that's a single doorway: the Department of Health and Human Services, Division of Licensing and Certification 2.
Here's the piece most people don't know. A behavioral health organization in Maine can hold a mental health license, a substance use disorder treatment license, or both 2. That last word matters. A program licensed only for substance use treatment is allowed to serve people with co-occurring mental health conditions, but it's not licensed to deliver mental health care as a primary service. The reverse is also true. The state rule that consolidates these requirements spells out which programs fall under which license and how integrated services are recognized 3.
So when you call a program in the South Portland area, ask plainly: What licenses does your facility hold through Maine DHHS? A truly integrated program will name both — or describe how its mental health services are delivered and supervised under a clearly licensed structure. A program that fumbles the question, or names only one license while promising full dual diagnosis care, is telling you where its actual capacity ends.
You can also verify directly. The DHHS Division of Licensing and Certification publishes its licensed behavioral health organizations, and a quick check confirms what you heard on the phone 2. That two-minute step protects you from marketing language that outruns the license on the wall.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Outpatient, PHP, or residential: matching level of care to your life
One of the biggest myths about co-occurring disorders is that they always require residential treatment. Sometimes they do. Often they don't. The honest answer depends on what your days look like, how stable your housing and supports are, and what a structured assessment shows about your medical and psychiatric needs.
That structured assessment has a name: ASAM Criteria. It's the framework used across the country to match a person to the right level of care — standard outpatient, intensive outpatient (IOP), partial hospitalization (PHP), or residential — based on factors like withdrawal risk, mental health stability, living environment, and readiness to engage 10. A program that takes co-occurring care seriously will run this assessment before placing you, not after.
Here's the rough shape of the options. Standard outpatient typically means a few hours a week and works when you're medically stable and have solid supports at home. IOP usually runs nine to fifteen hours a week across several days, with morning, afternoon, or evening tracks so you can keep working or caregiving. PHP is the most structured outpatient step — closer to twenty or more hours a week — for people who need daily contact but can sleep at home safely. Residential is the right call when withdrawal is dangerous, psychiatric symptoms are acute, or home isn't a safe place to recover.
For many people with co-occurring conditions who are working, parenting, or holding a household together, a trauma-informed IOP or PHP — with integrated dual diagnosis care and medication-assisted treatment when appropriate — is a legitimate and often preferable starting point. Ask any program: How does ASAM Criteria shape my placement, and what triggers a step up or step down? A clear answer means your level of care is being matched to your life, not to whatever bed happens to be open.

Cost, insurance, and time off: the practical questions to ask
Money and time are real. They're allowed to be part of this decision.
Most commercial insurance plans in Maine cover dual diagnosis treatment when it's medically necessary, and a capable program will run your benefits before your first session so you know what you're walking into. Ask three things directly: What does my plan cover for IOP, PHP, and outpatient care? What will my out-of-pocket cost look like per week? And what happens if my level of care changes mid-treatment? A program that handles intake well will give you specifics, not a shrug.
If you're working or caregiving, ask about scheduling before anything else. Programs designed for adults with daily responsibilities offer morning, afternoon, and evening tracks so treatment fits around a job or a kid's school pickup, not the other way around. That flexibility is part of what makes outpatient dual diagnosis care a workable option for people who can't pause life for thirty days.
Ask too about care coordination — whether someone on the team helps you communicate with your employer using protected language, sort out FMLA paperwork if you need it, and connect with outside prescribers or primary care. That kind of practical support often decides whether treatment actually starts.
A 20-minute phone consult worksheet you can score yourself
You don't need to remember every question on the call. You need a short, scoreable list you can keep in front of you. Here's one. Give each answer 0, 1, or 2 points: 0 for vague or evasive, 1 for partial, 2 for specific and confident.
- Do you screen every new client for both substance use and mental health conditions at intake? A specific yes — with named tools or a structured assessment — gets 2 points 5.
- Do you use ASAM Criteria to decide my level of care? Listen for an actual description of how the assessment shapes placement, not just a yes 10.
- Has your program been assessed using DDCAT or DDCMHT, and what did the results show? A program that knows its score — or names the domains it has been working on — earns the full 2 1.
- Is your team trained in the IDDT model, and how does that show up in my weekly sessions? Look for a concrete example, not a brochure phrase 4.
- Will one team hold both my diagnoses on one treatment plan, and how often does that team meet about my care?
- What licenses does your facility hold through Maine DHHS? A clear answer naming mental health, substance use, or both is a 2 2.
- How do you handle medication-assisted treatment alongside therapy for co-occurring conditions?
- What does care coordination look like if I'm working or caregiving — scheduling, employer paperwork, outside providers?
Eight questions. Sixteen points possible. A score of 12 or higher means you're talking to a program that can probably hold both halves of what you're carrying. Anything under 8 means keep dialing. Between those numbers, ask follow-up questions on the answers that felt thin.
One more thing — trust how the call feels. A program that takes co-occurring care seriously will sound calm, curious, and unhurried. If you feel rushed off the phone, that's information too.
What 'whole person' should actually mean — including the parts programs forget
“Whole person care” is on every brochure. Ask what it actually includes.
A real integrated program treats your substance use, your mental health, and the body those two live in. That means medication management coordinated with therapy, primary care connections, sleep, and yes — nicotine. Tobacco use is the most common substance among people in behavioral health treatment, and the CDC has flagged real gaps in cessation services at SUD and mental health facilities 11. If a program never asks whether you smoke or vape, it's missing a piece of the same picture.
Trauma fits here too. Trauma-informed care isn't a poster in the lobby — it's how staff handle hard moments, how groups are run, and whether your history shapes the plan instead of getting filed under “background.”
So ask: What do you screen for beyond drugs and mood — trauma, nicotine, sleep, primary care? The answer tells you how wide the program's definition of whole person actually goes.
Bringing it together: your next call
You started this looking for a program near you. You're ending it with a different kind of map — one that lets you tell, in a single phone call, whether a program can actually hold both halves of what you're carrying.
Pick up the phone with your worksheet next to you. Listen for screening that asks about both substance use and mental health, a placement process built on ASAM Criteria, one team holding one plan, and clear answers about Maine licensing. Trust how the call feels.
If you're in the South Portland area and want help sorting through options, Coastal Recovery Partners offers recovery planning and care coordination to walk you through what fits — no pressure, just a real conversation. You've already taken the hardest step. The next call is just one more.

Frequently Asked Questions
What's the difference between a dual diagnosis program and a regular rehab?
A regular rehab focuses on substance use. A dual diagnosis program is built to treat substance use and a mental health condition together, on one plan, by one team. Federal treatment guidance describes this as integrated care that “addresses all of a client's diagnoses and symptoms within one service system” 6. If only one half is being treated, you're in regular rehab.
How do I know if a program treats both conditions together instead of separately?
Listen for one team, one treatment plan, and screening that asks about both substance use and mental health at intake 5. Ask whether the program has been assessed using DDCAT or DDCMHT and what it scored — a score of 3 or higher means dual diagnosis capable 9. Vague answers about “working with outside providers” usually point to parallel care, not integrated care.
Do I need residential treatment, or can outpatient work for co-occurring disorders?
It depends on what a structured assessment shows, not on the diagnosis alone. ASAM Criteria is the framework programs use to match you to the right level of care based on withdrawal risk, psychiatric stability, and home environment 10. Many adults with co-occurring conditions do well in trauma-informed IOP or PHP. Residential is the right call when symptoms are acute or home isn't safe.
What questions should I ask during a phone consult with a treatment center?
Ask whether they screen every new client for both substance use and mental health 5, whether they use ASAM Criteria for placement 10, and whether their team is trained in the IDDT model 4. Ask which Maine DHHS licenses the facility holds 2. Ask who sits on your treatment team and how often they meet about your care. Specific answers matter more than reassuring ones.
Will insurance cover dual diagnosis treatment in Maine?
Most commercial plans in Maine cover dual diagnosis treatment when it's medically necessary, and a capable program will run your benefits before your first session. Ask what's covered for IOP, PHP, and standard outpatient, what your weekly out-of-pocket cost looks like, and what happens if your level of care changes mid-treatment. A program that handles intake well will give you specifics, not a shrug.
If a previous treatment didn't work, does that mean dual diagnosis care won't work either?
No. A previous episode often didn't hold because only one condition was being treated, or because two teams were running on parallel tracks that never met 6. That's a structural problem with the care, not a verdict on you. An integrated program changes the setup — one team, one plan, both diagnoses in the same room. Many people find traction the second time for exactly that reason.
References
- [PDF] Dual Diagnosis Capability in Addiction Treatment (DDCAT) Toolkit. https://www.dpbh.nv.gov/siteassets/programs/clinicalsapta/dta/partners/certification/DDCAT_Toolkit.pdf
- Behavioral Health - Division of Licensing and Certification - Maine.gov. https://www.maine.gov/dhhs/dlc/licensing-certification/behavioral-health
- C.M.R. 10, 144, ch. 123, PURPOSE AND APPLICABILITY. https://www.law.cornell.edu/regulations/maine/C-M-R-10-144-ch-123-PURPOSE-AND-APPLICABILITY
- IDDT Fidelity Scale | Center for Evidence-Based Practices. https://case.edu/socialwork/centerforebp/resources/iddt-fidelity-scale
- Chapter 3—Screening and Assessment of Co-Occurring Disorders. https://www.ncbi.nlm.nih.gov/books/NBK571017/
- Chapter 7—Treatment Models and Settings for People With Co-Occurring Disorders. https://www.ncbi.nlm.nih.gov/books/NBK571024/
- Managing Life with Co-Occurring Disorders - SAMHSA. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- Treatment Guidelines for Substance Use Disorders and Serious Mental Illnesses. https://pmc.ncbi.nlm.nih.gov/articles/PMC3285548/
- Dual Diagnosis Capability in Mental Health and Substance Use Treatment Programs. https://pmc.ncbi.nlm.nih.gov/articles/PMC3655772/
- ASAM Criteria for Patients with Addiction and Co-occurring Conditions. https://www.samhsa.gov/resource/ebp/asam-criteria-patients-addiction-co-occurring-conditions
- Tobacco-Related Clinical Services and Tobacco-Free Policies in Behavioral Health Treatment Facilities. https://www.cdc.gov/mmwr/volumes/74/wr/mm7414a3.htm
- Integrating Mental Health and Addiction Treatment into General Health Care. https://pmc.ncbi.nlm.nih.gov/articles/PMC7606646/
- Dual diagnosis capability in mental health and addiction treatment programs. https://pmc.ncbi.nlm.nih.gov/articles/PMC3594447/



