
Choosing Between Local Drug Rehab Centers

Key Takeaways
- Match treatment intensity to your medical needs, mental health, and home support rather than assuming inpatient is automatically better than outpatient care.7
- Learn the ASAM continuum so you can recognize where outpatient, intensive outpatient, and partial hospitalization fit and walk into intake calls informed.16
- Verify five things on intake calls: a real assessment, named evidence-based therapies, medication access, care coordination, and family involvement options.5,17
- Maine's geography shapes what programs offer, so ask directly about counselor credentials, wraparound services, and on-site medication for opioid use disorder19,9
- Use the eight-question list on first calls to separate programs that can explain their clinical thinking from those selling amenities.8
- Get clear answers about insurance coverage, out-of-pocket costs, and sliding-scale options before committing, and use SAMHSA's helpline if you need a neutral starting point.10
- Coastal Recovery Partners offers PHP, IOP, and outpatient under one roof in South Portland, allowing step-ups and step-downs without changing clinicians.1
Start with the question most rehab websites skip
If you're reading this, you've already done something difficult. Searching for a local drug rehab center, between work shifts or late at night, takes a kind of quiet courage that most people will never see. So before you compare a single program, take a breath. You don't have to figure this out alone, and you don't have to figure it out perfectly today.
Here's the question most rehab websites won't ask you: what level of care actually fits your life right now? Not what sounds the most serious. Not what a glossy photo of a beachfront facility suggests. The right starting point is matching treatment intensity to your medical needs, mental health, and the support you have at home — a principle that decades of addiction research keep coming back to. A 28-day inpatient stay isn't automatically better than a Tuesday-evening outpatient group. It's just different, and it's meant for different situations.7
Recovery is rarely a single event. It's ongoing care that adjusts as you do. That reframe matters, because it changes what you're shopping for. You're not looking for a building to fix you. You're looking for a program that will assess you honestly, offer therapies that actually have evidence behind them, coordinate with the rest of your health care, and stay flexible as your needs change. The rest of this guide will walk you through how to tell which local programs do that — and which ones just have good marketing.2
The level-of-care decision: where outpatient actually fits
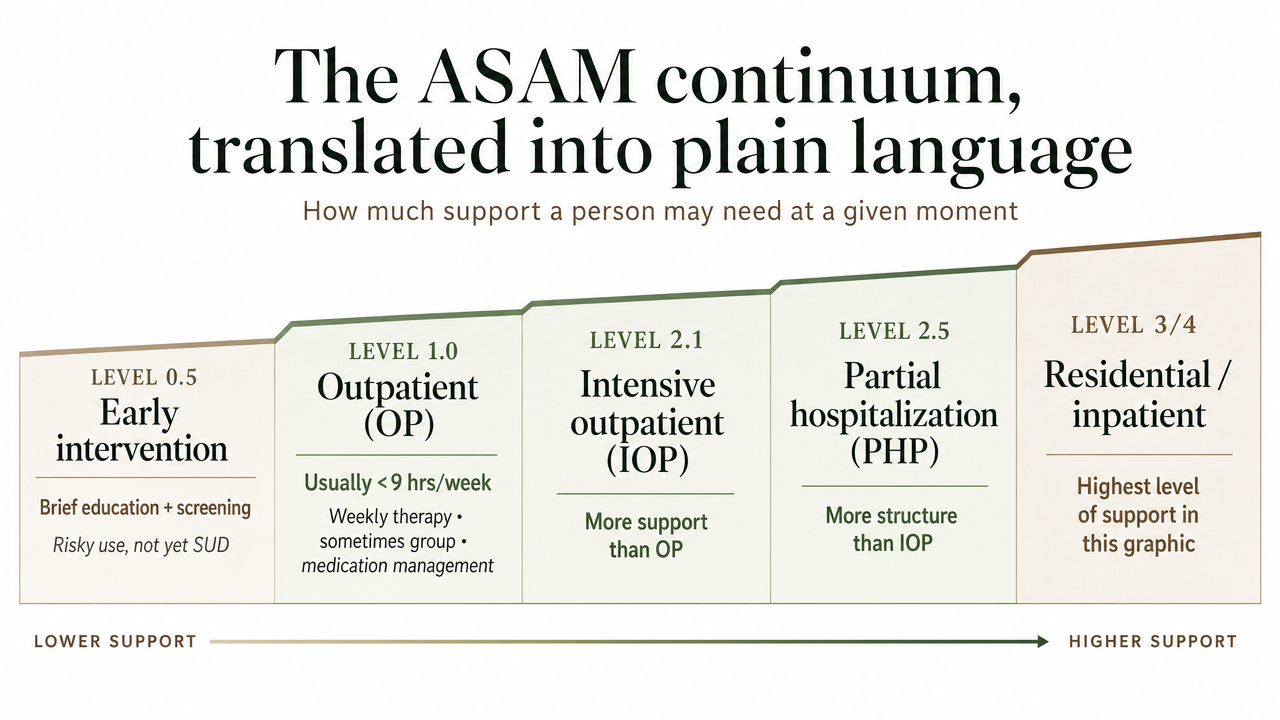
The ASAM continuum, translated into plain language
Most rehab websites throw around words like "intensive" and "comprehensive" without telling you what they actually mean. The American Society of Addiction Medicine (ASAM) cuts through that with a five-level continuum that states, insurers, and clinicians use to talk about how much support a person needs at a given moment. Once you can name where you might fit, every conversation with a local program gets easier.16
Here's the plain-language version of those five levels:16
- Level 0.5 — Early intervention. Brief education and screening for people whose use is risky but who don't yet meet criteria for a substance use disorder. Think a few counseling sessions, not a program.
- Level 1.0 — Outpatient (OP). Usually fewer than nine hours of treatment a week for adults. Weekly individual therapy, sometimes a group, and medication management if needed. Good fit when life is reasonably stable and you need ongoing support.
- Level 2.1 — Intensive outpatient (IOP). Nine or more hours a week, typically three sessions of group plus individual work. You sleep at home, keep your job, and treatment becomes a real part of your week.
- Level 2.5 — Partial hospitalization (PHP). Twenty or more hours a week of structured clinical care, often five days a week, with medical and psychiatric oversight. You go home at night but spend the workday in treatment.
- Levels 3.x and 4.0 — Residential and medically managed inpatient. 24-hour care for people who need a safer environment, complex withdrawal management, or stabilization that can't happen at home.
Levels 1.0, 2.1, and 2.5 are the outpatient band. That's where most adults who are working, parenting, or living with family land when they're matched honestly to their needs. Knowing which one you're being recommended for — and why — is one of the most useful things you can walk into an intake call already understanding.
Why outpatient is a matched choice, not a downgrade
Somewhere along the way, a lot of us picked up the idea that "real" rehab means leaving home for a month. That's not what the research says. The principle that runs through decades of addiction treatment science is matching — treatment intensity, duration, and mix of services should fit the person, not the other way around. Effective care often combines behavioral therapies and medication, monitored and adjusted over time, in whatever setting can actually deliver them.7,17
Outpatient programs at Levels 1.0, 2.1, and 2.5 are designed to do exactly that, with one specific advantage: you keep practicing recovery in the life you actually live. The Tuesday-evening IOP group, the morning PHP block before you pick up your kids, the standing Thursday check-in with your counselor — those aren't watered-down versions of inpatient. They're a different tool, and for many adults, a better-matched one. You're learning coping skills in the same kitchen where the cravings show up.
This also lines up with how recovery actually unfolds. It's rarely one episode and done; it's ongoing care that flexes as you do. A well-run local program can step you up to PHP during a hard stretch and back down to weekly outpatient as things stabilize, without you having to start over somewhere new. That continuity is the point. If a program can offer it, outpatient isn't a consolation — it's the right level of care, doing the right work, at the right time.2
Five things you can actually verify on an intake call
A real assessment, not a sales conversation
The first phone call tells you a lot. If the person on the other end spends ten minutes describing the building and two minutes asking about you, that's worth noticing. A good intake conversation feels more like a careful medical screening than a tour pitch. Someone should be asking about what you're using and how often, your physical and mental health history, any past treatment, what your home and work life look like, and what kind of support you have around you. That's the raw material a clinician needs to recommend a level of care honestly.
Decades of research are clear that treatment has to be matched to the individual and adjusted over time — not chosen off a menu. Good programs treat assessment as ongoing. They reassess as things change, because what fits in week one may not fit in week eight. You can ask directly: "How will you decide which level of care I need, and how often will that decision get revisited?"7,8
If the answer is vague, or if a program recommends a specific level of care before they've really asked about you, that's a flag. A real assessment respects how much you've already lived through.
Evidence-based therapies, named specifically
"Evidence-based" has become a phrase people put on websites without explaining what it means. You're allowed to ask what they actually do. SAMHSA's Evidence-Based Practices Resource Center exists precisely so that clinicians, communities, and patients can tell research-supported care apart from improvised programming. When you call a local center, ask which therapies they use by name and how they decide which one fits which person.5,11
Here is what a credible outpatient program should be able to describe in plain language, and what should make you slow down:5,7,11
- What you want to hear: cognitive behavioral therapy (CBT), motivational interviewing, relapse prevention work, contingency management for some substances, individual treatment planning, integration with medication when appropriate, and care for co-occurring mental health conditions.
- What should make you pause: a single curriculum that everyone walks through in the same order, no option for medication, no answer when you ask how they handle depression or anxiety alongside substance use, or detox framed as a complete solution rather than a starting point.
Therapies should also be tailored. NIDA is direct that the mix of behavioral therapy and medication should depend on the person and the substance, not on a fixed program template. If you ask, "How would you adjust this for someone with my history?" and you get a real answer — not a brochure paragraph — that's a good sign. You're looking for a clinician who can explain their thinking, not a script.11
Medication for addiction treatment: access, not ideology
If opioids or alcohol are part of your story, medication should be on the table. Medication for addiction treatment — sometimes called medication-assisted treatment, or MAT — means using medicines like buprenorphine, methadone, or naltrexone alongside therapy to reduce cravings, prevent withdrawal, and lower the risk of overdose. The research is settled enough that NIDA lists the combination of medication and behavioral therapy as one of the core principles of effective addiction care.7,17
And yet not every local program offers it, or talks about it the same way. Some still treat medication as a backup plan or a sign that someone "isn't really sober." That framing isn't supported by the evidence. When you call, ask plainly: "Do you prescribe medication for addiction treatment on-site, or do you coordinate with a prescriber who does?" Either answer can be fine. What matters is that the door is open and the program treats medication as a clinical decision, not a moral one.
You can also ask how they'd handle a transition — for example, if you're already on buprenorphine through your primary care doctor, or if you'd want to start during treatment. A program that can step you up to PHP, keep your medication steady, and step you back to weekly outpatient without disruption is doing the kind of continuity work the CDC and federal agencies are pushing toward.2
Care coordination as a clinical feature
Treatment that sits in a silo doesn't hold up well. You probably have a primary care doctor, maybe a therapist or psychiatrist, possibly a prescriber managing other medications, and a life with people in it. A good local rehab program treats coordinating with all of that as part of the clinical work, not an afterthought. The U.S. Surgeon General's report on substance use and health care systems makes the case bluntly: integration across primary care, mental health, and addiction treatment is one of the clearest levers we have for better outcomes.18
What does that look like in practice? Ask whether the program will, with your permission, talk to your primary care doctor. Ask if they communicate with outside psychiatrists or therapists you already trust. Ask how they handle referrals if you need a higher level of care for a stretch, or step-down support as you stabilize. Ask who on staff actually owns that coordination — a case manager, a clinician, someone else.1
A program that shrugs at these questions is asking you to be your own care coordinator at the hardest moment of your life. A program that has answers — names, processes, release-of-information forms ready — is offering you something real. That kind of connective tissue is what keeps recovery from being a series of disconnected episodes.
Family involvement, treated as part of treatment
For a lot of people, family is part of what makes recovery possible — and sometimes part of what makes it hard. Either way, the people around you matter. SAMHSA points to family therapy and family support as practices that can improve treatment effectiveness, not soft extras tacked onto the end. A program that offers family education sessions, family therapy, or even a clear plan for how loved ones can be looped in is taking that seriously.13
You don't have to know yet what you want from family involvement. Maybe you want a partner included in some sessions. Maybe you want a parent to learn what to say and what not to say. Maybe you need space, and the work is helping a sibling understand why. All of that is legitimate. The conversations about how to talk to a loved one about treatment, and how to support them once they're in it, are part of what good programs help with.12
On the intake call, ask: "What does family involvement look like here, and what's available if I want it — or don't?" The answer should sound like a clinical choice you get to make, not a marketing line.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
The Maine context: what to ask given where you live
Southern and coastal Maine isn't quite rural, and it isn't Boston. That in-between geography matters when you're comparing local programs, because the resources available to a center in South Portland can look very different from one an hour up I-95, and both will show up in your search results.
A national assessment of rural treatment centers found that, on average, they have fewer highly educated counselors, offer fewer wraparound services like case management and vocational support, and provide less diverse specialized treatment options than their urban counterparts. That's not a knock on rural clinicians, many of whom are doing excellent work with thin staffing. It's a reminder that the variation between two programs forty minutes apart can be real, and you're allowed to ask about it directly.19
Medications for opioid use disorder add another layer. Peer-reviewed work on rural Northern New England has documented substantial barriers to buprenorphine and methadone access in this region, even as the need has grown. CDC has named expanding access to these medications as a high-impact strategy for preventing overdose deaths in rural communities. Translation: if opioids are part of your picture, ask the program point-blank whether they prescribe on-site, partner with a local buprenorphine or methadone prescriber, and how quickly someone can actually start.3,9
A few specific questions worth bringing to a Maine intake call: What are your counselors' credentials, and how many full-time clinicians do you have? Do you offer case management, help with transportation, or coordination with primary care? If I need medication for opioid or alcohol use disorder, can you start it here, and how soon? Do you have evening or weekend groups that work around a shift schedule? The answers will tell you which local program is built for the life you actually live.
The eight questions to ask before you commit
Print this list, or screenshot it on your phone. When you call a local program for the first time, you don't have to remember everything you've read — you just need a handful of questions that pull real information out of the conversation. These eight are the ones that tend to separate programs that can describe their clinical thinking from programs that can only describe their amenities.1,5,7,8,16,17,18
- How will you assess me, and what does that include? You're listening for a real screening — substance use history, mental health, physical health, home and work life, support system. Continuous assessment is a core principle of effective care, not a one-time intake checkbox.
- What level of care would you recommend, and why? A good answer references something close to the ASAM continuum — outpatient, intensive outpatient, partial hospitalization — and explains the reasoning out loud.
- Which specific therapies do you use? You want names: CBT, motivational interviewing, relapse prevention, contingency management. "Evidence-based" without specifics isn't an answer.
- Do you treat co-occurring mental health conditions in the same program? Depression, anxiety, trauma, and substance use travel together often enough that integrated care is a baseline expectation.
- Do you prescribe medication for addiction treatment, or coordinate with someone who does? For opioid or alcohol use disorder, this is not optional information.
- How do you coordinate with my primary care doctor or outside therapist? Integration with the rest of your health care is a quality marker, not a courtesy.
- How does treatment change if my needs change? Stepping up to PHP during a hard stretch, or down to weekly outpatient as things stabilize, should be a normal part of the plan.
- What does family involvement look like, if I want it? A clear answer — sessions, education, or none if you'd rather — tells you they've thought about it.
You don't owe anyone a decision on the first call. If a program answers these well, write that down. If they dodge, that's information too.
Cost, insurance, and the first phone call
Money is part of this, and pretending otherwise doesn't help anyone. On the first call, a good program will ask what insurance you have and walk you through what's likely covered before you've committed to anything. Outpatient visits, intensive outpatient, and partial hospitalization are commonly covered services across most plans, including Medicare, which covers outpatient mental health visits, partial hospitalization, and certain screenings and treatments for substance use disorders. If a program can't explain how your specific coverage applies — or won't put a benefits check in writing — that's a reason to slow down.4
Ask three plain questions: What will my insurance cover for the level of care you're recommending? What would I owe out of pocket per week or per month? If I'm uninsured or underinsured, what self-pay or sliding-scale options exist? Real answers, not ranges pulled from the air.
If you're not sure where to start, SAMHSA's National Helpline is free, confidential, and runs 24/7 at 1-800-662-HELP (4357), and can refer you to nearby programs that match your needs and coverage. It's a reasonable first call before you commit to anything.10
When the right choice is Coastal Recovery Partners
If you live in or near South Portland and outpatient care at Levels 1.0, 2.1, or 2.5 sounds like the right fit, Coastal Recovery Partners is built around exactly that band of the continuum. The program offers partial hospitalization, intensive outpatient, and standard outpatient care under one roof, so a step up during a hard week or a step down as life steadies doesn't mean starting over with a new clinician. Mornings, afternoons, and evenings are available, which matters when you're holding a job or caring for kids.1
The clinical model is trauma-informed and built on therapies the research actually backs — CBT, DBT, motivational interviewing, and relapse prevention work — with integrated care for co-occurring mental health conditions and medication for addiction treatment coordinated alongside therapy. Care coordination with your primary care doctor, outside prescribers, and family supports is treated as part of the work, not an extra.5,7,18
If you'd like a real conversation about what level of care fits, call. You can ask the eight questions above and decide from there.
Frequently Asked Questions
What's the difference between PHP, IOP, and standard outpatient care?
They're three points on the same continuum, separated mostly by hours and intensity. Standard outpatient (ASAM Level 1.0) is usually fewer than nine hours a week. Intensive outpatient (Level 2.1) is nine or more hours a week, often three group sessions plus individual work. Partial hospitalization (Level 2.5) is twenty or more hours a week with medical and psychiatric oversight, while you still sleep at home.16
Is outpatient rehab as effective as going to a residential program?
When the level of care is matched honestly to your needs, yes. Decades of research point to matching treatment intensity, duration, and services to the individual rather than defaulting to one setting. Outpatient lets you practice recovery in your actual life, with the same combination of behavioral therapy and medication that residential programs use. It's a different tool, not a lesser one.7,17
Do I have to stop using before I can start treatment at a local rehab center?
No. Be honest on the intake call about what you're using and how often. A good program assesses where you are and builds a plan from there, which may include medication for withdrawal or cravings alongside therapy. Detox on its own is rarely enough; ongoing treatment is what holds. Show up as you are.7,11
How do I know if a local program treats co-occurring mental health conditions?
Ask directly: "Do you treat depression, anxiety, trauma, or other mental health conditions in the same program, with the same team?" Listen for integrated care, not a referral out. Effective treatment addresses co-occurring conditions alongside substance use rather than in separate silos. A trauma-informed approach and named therapies like CBT, DBT, or motivational interviewing are good signs.5,7
What should I expect on the first phone call to a rehab center?
Expect questions about you, not a sales pitch. A real intake conversation covers what you're using, your physical and mental health, past treatment, home and work life, and what support you have. They should explain which level of care they'd recommend and why, check your insurance, and answer your questions in plain language. If you'd rather start with a neutral resource, SAMHSA's helpline is free and confidential at 1-800-662-HELP.10,8
Can my family be involved in my treatment, and should they be?
They can, and for many people it helps. SAMHSA points to family therapy and family support as practices that can improve treatment effectiveness, not extras. That might mean a partner joining some sessions, a parent attending education, or a sibling learning what to say. It might also mean space, and that's a legitimate choice too. Ask what family involvement looks like, and what's available if you want it.12,13
References
- Chapter 5—Specialized Substance Abuse Treatment Programs. https://www.ncbi.nlm.nih.gov/books/NBK64815/
- Treatment of Substance Use Disorders | Overdose Prevention. https://www.cdc.gov/overdose-prevention/treatment/index.html
- Opioid Use Disorder: Rural Policy Brief. https://www.cdc.gov/rural-health/php/policy-briefs/opioid-overdoses-policy-brief.html
- Mental health & substance use disorders. https://www.medicare.gov/coverage/mental-health-substance-use-disorder
- Evidence-Based Practices Resource Center. https://www.samhsa.gov/libraries/evidence-based-practices-resource-center
- Evidence-Based Practices Resource Center (Healthy People 2030). https://odphp.health.gov/healthypeople/tools-action/browse-evidence-based-resources/evidence-based-practices-resource-center
- Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- Foundational Principles of Substance Use Disorder (SUD) Treatment. https://case.edu/socialwork/centerforebp/sites/default/files/2024-03/Foundational%20Principles%20of%20SUD%20Treatment_Final_1.9.24.pdf
- The Opioid Epidemic in Rural Northern New England. https://pmc.ncbi.nlm.nih.gov/articles/PMC6879818/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Treatment Approaches for Drug Addiction DrugFacts. https://nida.nih.gov/publications/drugfacts/treatment-approaches-drug-addiction
- How to Talk to Someone About Help For Mental Health & Substance Use. https://www.samhsa.gov/find-support/helping-someone/how-to-talk-to-someone-about-help
- Helping Families Cope with Mental Health and Substance Use. https://www.samhsa.gov/mental-health/children-and-families/coping-resources
- Prevention of Drug Use and Treatment of Drug Use Disorders in Rural Settings. https://digitalcommons.usm.maine.edu/cgi/viewcontent.cgi?article=1023&context=behavioral_health
- Frequently Asked Questions - SAMHSA. https://www.samhsa.gov/about/faqs
- Overview of Substance Use Disorder (SUD) Care Clinical Guidelines: ASAM Resource Guide. https://www.medicaid.gov/state-resource-center/innovation-accelerator-program/iap-downloads/reducing-substance-use-disorders/asam-resource-guide.pdf
- Principles of Drug Addiction Treatment: Questions and Answers. https://nida.nih.gov/sites/default/files/podat_1.pdf
- Health Care Systems and Substance Use Disorders (U.S. Surgeon General’s Report). https://www.ncbi.nlm.nih.gov/books/NBK424848/
- Rural substance use treatment centers in the United States: an assessment. https://pmc.ncbi.nlm.nih.gov/articles/PMC4775429/



