
Steps to Finding a Local Rehab That Fits Your Life

Key Takeaways
- Begin by mapping your real weekly schedule before researching programs, because the hours you can realistically commit to treatment determine which level of care will actually work.
- Match clinical intensity to your situation honestly: too-intense programs collapse under real-life demands, while too-light options can't hold serious problems, making the middle path often the right fit 5.
- Use FindTreatment.gov and the SAMHSA Helpline at 1-800-662-HELP to build your list, then verify each program against Maine DHHS Behavioral Health licensing before calling 31112.
- Treat the intake assessment as a 60–90 minute placement conversation, not a test, where honesty about use and schedule helps the clinician match you to the right setting 4.
- Walk away from any program that won't screen for mental health and trauma alongside substance use, since integrated 'no wrong door' care is what the evidence supports 9.
- Outpatient often fits a working life better and costs less per episode, while still building relapse-management skills inside the environment where triggers actually happen 610.
- Use the first phone call to confirm licensing, levels of care, assessment scope, group times, attendance policies, medication options, and costs before committing to anything 23.
- Plan the conversations around treatment too — work disclosures, family support, and Maine winter attendance — so logistics outside the clinic don't derail the work inside it 710.
Start where you actually are: a working adult in Greater Portland
If you're reading this on your phone at 11:47 p.m., or in your car in a parking lot off Broadway before you go back inside — you already know something has to change. You don't need a lecture about that. You need a plan that doesn't blow up the rest of your life to get you better.
Here's the honest part: most people searching "local rehab" picture a place in the woods with a 30-day stay, a packed suitcase, and an awkward conversation with their boss. That picture is one option. It is not the only option, and for a lot of working adults in South Portland, Scarborough, Westbrook, and the rest of Greater Portland, it isn't even the right one. SAMHSA's own guidance starts in the same place you're starting — with the simple acknowledgment that figuring out where to go for help with alcohol or drugs can feel overwhelming, and that there are real, accessible ways to begin 1.
So before you scroll through fifty websites that all look the same, take a breath. The goal of this article isn't to sell you on a building. It's to help you ask better questions: What does my actual week look like? What level of care matches what I'm dealing with? Who in this state is licensed to deliver it? You're going to make a few phone calls and a few small decisions. That's it for now. You're already further along than you were an hour ago, and that counts.
What does your Tuesday actually look like?
Forget the brochure language for a minute. Picture an ordinary Tuesday. What time does your alarm go off? Who needs to eat breakfast besides you? When do you start work, and when can you actually leave? Is there a pickup at 3:15? A second shift? A standing thing on Wednesday nights you cannot miss?
That picture — your real week, not an idealized one — is the thing that decides which level of care will actually work. Most people start by asking "how serious is my problem?" That's the wrong first question. The first question is, "how many hours per week can I give to treatment without the rest of my life falling apart?" Then you match the clinical level to that answer, with help from a professional who can tell you if your honest hours are enough for what you're dealing with.
Here's the simple version of the ladder, the one SAMHSA describes in plain terms 2:
- Standard outpatient is regular office or telehealth visits — usually one to a few hours a week. You keep your job, your school pickups, your evenings.
- Intensive outpatient, or IOP, is the middle rung: roughly nine or more hours a week, broken into a few group sessions plus individual therapy, often offered in morning, afternoon, or evening blocks so working adults can actually attend 210.
- Partial hospitalization (PHP) is closer to twenty hours a week — think a part-time job's worth of clinical care during the day, while you still go home to sleep in your own bed.
- Residential is everything else on pause while you live on-site.
So before you start calling places, take five minutes and write down what your Tuesday actually looks like — and Wednesday, and Saturday. Circle the hours that are truly fixed. Look at what's left. That blank space is where treatment fits. A good local program will build a schedule around that blank space, not ask you to invent more of it.
The two ways people choose wrong
There's a quiet trap on either side of this decision, and it's worth naming both before you call anyone.
The first trap is picking a program that's too intense for what your week can hold. You panic, you book a 30-day residential bed three hours away, you tell your manager you have a family emergency — and somewhere around day eleven, the math of your real life catches up. The mortgage. The kids. The job you actually need to come back to. You leave early, feel like you failed, and now you're carrying shame on top of everything else. Treatment that doesn't fit your life doesn't get finished, and unfinished treatment is its own setback.
The second trap is the opposite. You pick the lightest possible option because it barely disrupts anything — one therapy hour a week, maybe a support group on Thursdays — when what you're actually dealing with needs more structure than that. Cravings hit on a Saturday night and there's no one to call. The hour of therapy can't hold the weight. You relapse, and the story you tell yourself is that treatment doesn't work. It does. That dose of it just wasn't enough for what you brought in.
This is why patient-treatment matching matters more than picking the fanciest building. Research on matching services to actual patient needs shows real improvement in outcomes when the level of care lines up with what someone is dealing with — and the gap is widest for higher-need patients who get under-served 5. The middle path exists for a reason. Intensive outpatient was designed exactly for this — enough hours and enough structure to hold a serious problem, without taking your whole life off the table 10.
Use the locators, then verify what they tell you
Two free tools will save you hours of guesswork. The first is SAMHSA's FindTreatment.gov, a confidential search you can run by state, county, and distance from your zip code — filter for substance use, set the radius to whatever you can realistically drive after a workday, and start a list 11. The second is the SAMHSA National Helpline at 1-800-662-HELP (4357), free and confidential, 24/7, in English and Spanish, staffed by people whose only job is to point you toward treatment in your area 8. If you've been staring at search results for an hour, call. They will not lecture you. They will not ask for your insurance card before they talk to you.
Now the part most articles skip. The federal locator is a starting point, not a verdict. A government audit of SAMHSA's locator flagged real concerns about how facility information gets verified, and recommended annual validation of a sample of listings to catch outdated or incomplete entries 12. Translation: a program showing up on the map doesn't automatically mean it's currently operating, currently licensed, or offering what the listing says it offers. Don't skip the next step.
For Maine, that next step is the DHHS Division of Licensing and Certification. The Behavioral Health Program licenses both Mental Health and Substance Use Disorder programs in the state — that's the official record of who is allowed to operate a SUD outpatient program here 3. Before you call any facility on your list, take five minutes to confirm the program name appears on Maine's licensing rolls. If it doesn't, that's your answer.
Once you've cross-checked the locator against state licensing, build a short pre-call checklist you can keep on your phone. Six items cover most of what matters:
- Confirm the Maine DHHS Behavioral Health license
- Confirm independent accreditation
- Ask whether they offer medication-assisted treatment if that's relevant to you
- Ask how they handle co-occurring mental health conditions like anxiety, depression, or PTSD
- Ask whether they have evening or early-morning groups for working adults
- Confirm what your insurance covers, plus self-pay rates if you'd rather keep insurance out of it 13
Screenshot the list. You're not being difficult by asking — you're doing exactly what someone choosing a doctor for any other serious condition would do. The programs that answer these questions clearly and without defensiveness are the ones worth keeping on your shortlist.
The assessment is a long conversation, not a test
The word "assessment" sounds clinical and a little terrifying, like you're about to be graded on how bad things have gotten. It isn't that. A real intake assessment is a long, careful conversation — usually somewhere between 60 and 90 minutes — where a clinician asks about your history with substances, your physical health, your mental health, what's going on at home and at work, what you've already tried, and what you actually want your life to look like. There's no passing or failing. There's just a more accurate picture at the end of it than you walked in with.
NIH treatment planning guidance is direct on this point: a good plan starts by assessing severity and any co-occurring conditions, then matches you to the appropriate setting from there 4. That's the whole purpose of the conversation. The clinician is trying to figure out, with you, whether standard outpatient is enough, whether intensive outpatient is the right fit, or whether you need a higher level of care first — maybe a few days of medical detox — before stepping down. You are not being interrogated. You are being placed.
Two things help make this conversation worth your time. The first is honesty about how much you're actually using, how often, and how it's affecting work, sleep, relationships, and your body. Underselling it to look better gets you a plan that's too light. The second is honesty about what your week can hold — the same Tuesday picture you already sketched. The clinician needs both halves to do their job.
You can also ask questions back. How will you reassess if I'm struggling? What happens if I need to step up or step down? Patient-treatment matching isn't a one-time decision; it's something a good program revisits as your situation changes 5. Walking out of an assessment with a plan you understand — and the name of one person you can call when something feels off — is what a useful first appointment looks like.
Why the program needs to ask about trauma and mental health on day one
If a program treats your substance use without ever asking about your mental health or what you've lived through, walk out. That sounds harsh, but it's the single biggest reason people relapse out of treatment that looked good on paper. Most adults who show up for help with drinking or drugs are also carrying something else — anxiety that's been there since middle school, a depression that got heavier after a loss, a trauma history that the drinking was quietly managing. Treating one half and ignoring the other half is like bailing water out of a boat without patching the hole.
SAMHSA frames this as the "no wrong door" principle: someone showing up for mental health care should get screened for substance use, and someone showing up for substance use should get screened for mental health conditions, every time 9. Integrated care — where the same team addresses both at once — is what the evidence supports. You should not have to coordinate two separate clinics that don't talk to each other while you're trying to keep your job and not drink on a Friday night.
So here's what to listen for during that first call or assessment:
- Does the clinician ask about trauma in a careful, matter-of-fact way — not demanding details, just asking whether it's part of the picture?
- Do they ask about anxiety, depression, sleep, panic, intrusive thoughts?
- Do they describe their therapy as trauma-informed, and can they explain what that actually means in plain language — things like pacing, choice, predictability, not being asked to retell the worst day of your life on day one?
- Do they offer therapies designed to hold both sides at once, like CBT and DBT integrated with relapse prevention?
If the answer is yes across the board, you're in the right kind of room. If the program treats your mental health as something to deal with "after you get sober," that's the wrong door, even if it's two miles from your house.
Why outpatient often fits a working life
Here's the part nobody tells you when you're scared and Googling: the cheaper option is often also the one that lets you keep your life. That's not a sales pitch — it's what the cost research actually shows.
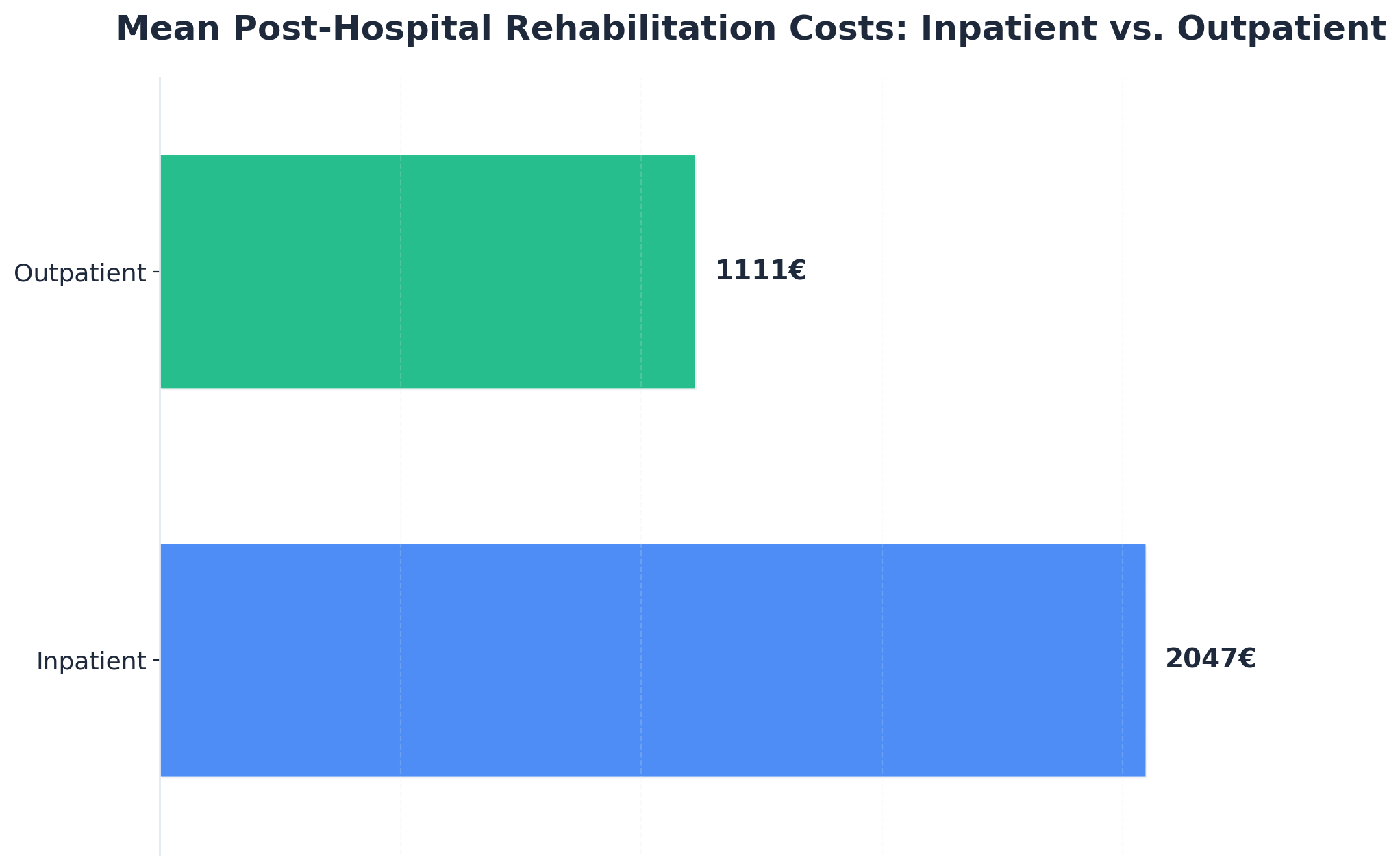
One peer-reviewed comparative cost analysis put mean per-episode rehabilitation costs at roughly €1,111 for outpatient versus €2,047 for inpatient, with the authors describing outpatient as economically superior on a per-episode basis 6. A few honest caveats: the study compared rehabilitation episodes in a European healthcare context, not Maine billing, and the headline finding was about cost — outcome comparability between the two settings is something the researchers themselves treat carefully, not as a blanket equivalence. So don't read it as "outpatient always works as well as inpatient." Read it as: when outpatient is the appropriate level of care for what you're dealing with, it tends to deliver that care at meaningfully lower cost per episode.
That matters for a working adult in Greater Portland for reasons that go beyond the invoice. The dollars-per-episode gap is the visible cost. The invisible costs of inpatient — the unpaid leave, the childcare scramble, the explanation to a manager, the catch-up backlog when you return — are real and they fall on you. Outpatient keeps those costs from stacking on top of the clinical bill.
There's also a clinical argument for the working-life fit, not just an economic one. Intensive outpatient programs were specifically designed to establish psychosocial supports and build relapse-management and coping skills while you're still inside your regular environment — the same environment where the cravings, the triggers, and the Friday-night decisions actually happen 10. You're practicing recovery in the place you have to live it, with morning, afternoon, or evening groups built around real schedules. That's not a watered-down version of treatment. For a lot of people, it's the version that holds.
None of this means outpatient is right for everyone. If you need medical detox, or your home environment isn't safe enough to support recovery yet, a higher level of care comes first. The point is simpler: don't rule out the option that fits your week just because it costs less or doesn't look like the version of rehab you've seen on TV.
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
What to ask on the phone before you commit
The first call is usually the hardest part of the whole process. Your hands might be shaky. You might rehearse what to say and then forget it the second someone picks up. That's normal. The person on the other end has heard every version of this call, and a good intake coordinator will not make you perform calm to be taken seriously. You can say, "I'm not sure where to start, but I think I need help." That sentence is enough.
Once you're past the introductions, here are the questions worth asking before you book anything:
- Are you currently licensed by Maine DHHS for substance use disorder outpatient services, and what's your license status? 3
- What levels of care do you offer in-house — standard outpatient, intensive outpatient, partial hospitalization — and can you step me up or down if my needs change? 2
- Will my first appointment include a full assessment that looks at both substance use and mental health, or are those handled separately? 49
Then get specific about your week. What are your group times — do you actually have evening or early-morning options, or is that just on the website? How many days per week is IOP, and how long is each session? If I miss a session because of work or weather, what happens? Maine winters are not a hypothetical; ask how they handle attendance when 295 is a parking lot.
Cover medication and money before you hang up. Do you offer medication-assisted treatment on-site, or coordinate it with a prescriber? 2 What insurance do you take, what's my likely out-of-pocket, and what's the self-pay rate if I'd rather not run it through insurance? Can someone help me figure out the benefits part — that piece alone keeps people from calling back.
One last question, and it's the one that tells you the most: "What does your program do well, and what does it not do well?" A program that can answer that honestly is a program worth driving to. Take notes. You don't have to decide on the call.
The conversations outside the clinic: work, family, winter
Treatment is the easy part to schedule. The conversations around it are usually what people lose sleep over.
Start with work, because that's the one that probably scares you most. You don't owe your manager a diagnosis. Under most circumstances, you can simply say you're starting a medical appointment series and ask about adjusting hours, using PTO, or shifting to an evening schedule for a stretch. If your benefits include an Employee Assistance Program, that's often the quietest door — EAP conversations are typically confidential and separate from your HR file. A program that offers morning or evening IOP groups makes this conversation shorter, because you may not need a schedule change at all 210.
Family is its own decision. You don't have to tell everyone, and you don't have to tell anyone on day one. Pick the one or two people whose support actually helps — not the ones who'll have opinions — and tell them what you need: a ride on group nights, an hour of childcare, someone to text on a hard Saturday. Social support is part of how this works, not a bonus feature 7.
Then there's winter. Maine weather is going to test your attendance somewhere around late January, when 295 is slush and your group starts at 6 p.m. Ask the program upfront how they handle weather closures, whether they offer telehealth makeups, and what their attendance policy looks like when the storm is real. A program built for working adults in this state will already have an answer.
One concrete next step
You don't have to decide today which program you'll attend. You don't have to tell anyone yet. You just have to do one small thing before you close this tab.
Pick one of these:
- Open FindTreatment.gov, set the radius to a drive you can actually do after work, and write down three programs in Greater Portland that look possible 11.
- Or call the SAMHSA National Helpline at 1-800-662-HELP — free, confidential, 24/7, in English and Spanish — and let someone else help you make the list 8.
Either one takes about ten minutes.
Then tomorrow, cross-check those names against Maine DHHS Behavioral Health licensing, and make one phone call 3. That's it. One call, with the questions you already have on your phone.
If an intensive outpatient program built around evening or morning groups sounds like the version of help that could actually fit your week, Coastal Recovery Partners in South Portland is one of the doors worth knocking on. Whichever door you pick — knock on one this week.

Frequently Asked Questions
Can I go to rehab without quitting my job?
Often, yes. Standard outpatient and intensive outpatient programs are built around real schedules, with morning, afternoon, or evening groups so you can keep working while you get help 2. IOP typically runs about nine or more hours a week across a few sessions, designed to fit around employment rather than replace it 10. If your situation needs more structure first, a short higher level of care followed by a step-down to outpatient is another path worth asking about.
How do I check if a local rehab program is actually licensed in Maine?
Go straight to the Maine DHHS Division of Licensing and Certification. The Behavioral Health Program is the office that licenses both Mental Health and Substance Use Disorder programs in the state, and that's the official record you want to cross-check before booking anything 3. If you found the program through SAMHSA's FindTreatment.gov, treat that listing as a starting point — a federal audit recommended stronger annual verification of facility data, so confirm with state licensing too 12.
What's the difference between standard outpatient and intensive outpatient (IOP)?
Standard outpatient is usually a weekly therapy appointment or two — regular office or telehealth visits that fit easily around a job 2. Intensive outpatient is a step up: roughly nine or more hours per week, combining group sessions with individual therapy, designed to build psychosocial supports and relapse-management skills while you keep living at home 210. IOP is the middle path when one weekly therapy hour isn't enough but residential treatment is more than your week can hold.
Do I have to tell my family or employer that I'm getting treatment?
No. Treatment is confidential, and you decide who to tell and when. With your employer, you can usually frame it as a medical appointment series without disclosing a diagnosis, and an Employee Assistance Program is often a separate, private channel. With family, pick one or two people whose support actually helps — social support genuinely matters to outcomes 7 — and tell them only what you need them to know.
What if I have anxiety, depression, or trauma along with substance use?
That's the rule, not the exception, and a good program treats both at once. SAMHSA's "no wrong door" guidance says anyone showing up for substance use should be screened for mental health conditions, and vice versa, with integrated care as the standard 9. When you call, ask whether the assessment covers both 4, and whether they describe their work as trauma-informed. If they say mental health gets handled "after you get sober," keep looking.
What should I ask a rehab program before I commit to going?
Six questions cover most of it: Are you licensed by Maine DHHS for SUD outpatient services 3? What levels of care do you offer in-house, and can you step me up or down 2? Does intake assess both substance use and mental health 49? Do you have evening or early-morning groups? Do you offer or coordinate medication-assisted treatment? What will this cost with my insurance, or self-pay? A good program answers each one directly 1.
References
- Struggling with Addiction? Tips on Finding Quality Treatment. https://www.samhsa.gov/blog/struggling-addiction-tips-finding-quality-treatment
- Treatment Types for Mental Health, Drugs and Alcohol | SAMHSA. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Behavioral Health - Division of Licensing and Certification - Maine.gov. https://www.maine.gov/dhhs/dlc/licensing-certification/behavioral-health
- 4 Substance Abuse Treatment Planning - NCBI - NIH. https://www.ncbi.nlm.nih.gov/books/NBK572945/
- The effect of matching comprehensive services to patients' needs on .... https://pmc.ncbi.nlm.nih.gov/articles/PMC2761625/
- Comparative cost analysis of outpatient and inpatient rehabilitation .... https://pubmed.ncbi.nlm.nih.gov/18682412/
- Patient-Treatment Matching: Rationale and Results - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6876445/
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- Managing Life with Co-Occurring Disorders - SAMHSA. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- Substance Abuse Intensive Outpatient Programs: Assessing the Effectiveness and Costs. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- FindTreatment.gov (English) - SAMHSA. https://www.samhsa.gov/resource/dbhis/findtreatmentgov-english
- Audit of SAMHSA's Behavioral Health Treatment Services Locator. https://oig.hhs.gov/reports/work-plan/browse-work-plan-projects/audit-of-samhsas-behavioral-health-treatment-services-locator/



