
Outpatient Treatment vs Inpatient Treatment: Which to Choose?

Understanding Treatment Intensity Levels: Outpatient Treatment vs Inpatient Treatment
Outpatient Program Structures Explained
Outpatient care excels when you need to maintain your career and home life while receiving intensive, evidence-based support.
When evaluating outpatient treatment vs inpatient treatment, the right choice hinges on balancing your professional obligations with your clinical needs. Outpatient addiction treatment programs are structured to provide high-quality care while allowing you to continue meeting your daily professional and personal commitments. These programs are designed around varying levels of intensity, ranging from standard Outpatient (OP) sessions to Intensive Outpatient Programs (IOP) and Partial Hospitalization Programs (PHP), which can offer up to five sessions per week and several hours of clinical engagement per day.
At Coastal Recovery Partners in South Portland, Maine, we understand that stepping away from your career isn't always feasible. A defining feature of our outpatient treatment is its flexibility. Schedules are arranged to accommodate work hours—morning, afternoon, or evening sessions are common—making this approach highly practical for working professionals. Care typically includes individual and group therapy, medication-assisted treatment (MAT), relapse prevention strategies, and integrated dual diagnosis treatment for co-occurring mental health disorders.
The option to receive care while living at home and maintaining employment underscores why 71% of individuals inquiring about treatment express a preference for outpatient settings, citing work and family obligations as primary motivators. Another advantage is the ability to tailor care plans to the severity of substance use and mental health needs.5
"Treatment completion rates in outpatient settings improve by 23-31% when intensity is matched to clinical need, highlighting the importance of personalized care structures."6
Outpatient treatment vs inpatient treatment often comes down to this balance between clinical oversight and real-world flexibility for sustained recovery. Next, a closer look at inpatient care models will further clarify the full spectrum of treatment intensity options.
Inpatient Care Models and Components
Inpatient care excels when 24/7 medical supervision and immediate stabilization are the top priorities.
Inpatient treatment models offer the highest level of structure and clinical supervision in the addiction care spectrum. These programs require individuals to reside on-site throughout the course of care, providing round-the-clock monitoring, medical management, and a highly controlled environment. Inpatient care is particularly effective for those with severe substance use disorders, acute withdrawal risks, or co-occurring psychiatric conditions that cannot be safely managed in an outpatient setting.8
A typical inpatient program features a multidisciplinary team—including physicians, nurses, therapists, and peer support specialists—who collaborate to deliver an integrated care plan. Core components often include daily individual and group therapy, medication management when indicated, relapse prevention training, and psychoeducational workshops. Medical detoxification is available on-site for individuals requiring close observation during withdrawal, a critical distinction from outpatient options.2
The intensity of inpatient care supports stabilization during high-risk periods, with stays commonly ranging from two to six weeks. Research highlights that 60-80% of individuals entering inpatient programs present with complex dual diagnoses, reinforcing the need for comprehensive mental health resources alongside addiction treatment. Understanding the differences between outpatient treatment vs inpatient treatment helps professionals determine which setting best supports safety, stabilization, and engagement during the most acute phases of recovery.8
Clinical Factors Driving Treatment Placement
Severity Assessment and Co-Occurring Conditions
Inpatient treatment excels for acute, severe cases, while outpatient programs are highly effective for mild-to-moderate severity with stable mental health.
Severity of substance use disorder and the presence of co-occurring psychiatric conditions are the primary clinical factors influencing whether you will benefit more from outpatient or inpatient placement. In most scenarios, inpatient treatment is the preferred choice for individuals with severe addiction, active psychiatric instability, or a lack of safe, supportive environments. Research consistently shows that 60-80% of patients entering inpatient care have documented dual diagnoses, underscoring the need for integrated mental health and addiction services in these settings.8
Outpatient treatment excels in cases where substance use severity is moderate, psychiatric symptoms are stable, and you demonstrate reliable engagement with care. Programs such as Intensive Outpatient (IOP) and Partial Hospitalization (PHP) allow for comprehensive therapy—like Cognitive Behavioral Therapy (CBT) and Dialectical Behavior Therapy (DBT)—while supporting continued employment and community living. A meta-analysis of 47 studies found no significant difference in outcomes between well-matched outpatient and inpatient populations, provided placement aligns appropriately with clinical severity and dual diagnosis needs.9
The decision-making process relies on multi-dimensional assessment tools that evaluate substance use history, mental health status, risk of self-harm, and environmental supports. Proper placement can increase outpatient completion rates by up to 31% when the intensity of care matches clinical needs.6
Outpatient treatment vs inpatient treatment decisions should always integrate these clinical dimensions to ensure optimal placement. Next, the discussion will turn to how medical complexity and withdrawal management further shape placement recommendations.
Figure 1: Key clinical criteria guiding the placement decision between outpatient and inpatient care.
Medical Complexity and Withdrawal Management
Inpatient care excels for high-risk medical detox, whereas outpatient care is ideal for manageable withdrawal and ongoing medication-assisted treatment.
When evaluating medical complexity and withdrawal management, inpatient treatment offers distinct advantages for individuals with acute medical needs or high-risk withdrawal profiles. Inpatient programs are equipped to provide 24/7 medical supervision, immediate intervention for complications, and on-site detoxification services. This setting is especially critical for substances like alcohol, benzodiazepines, and opioids, where withdrawal can lead to life-threatening complications or require medication titration under close observation. Research supports that inpatient detoxification is recommended for those with unstable vital signs, severe comorbidities, or a history of complicated withdrawal episodes.8
What is Medication-Assisted Treatment (MAT)?
MAT is an evidence-based approach that combines FDA-approved medications with counseling and behavioral therapies to treat substance use disorders. At Coastal Recovery Partners, our coordinated MAT programs provide pharmacological support alongside therapies like CBT and DBT to treat the "whole patient," significantly reducing cravings and the risk of relapse.
Outpatient programs, including IOP and PHP, can successfully manage withdrawal in cases where symptoms are expected to be mild to moderate and you have medical stability. Outpatient Medication-Assisted Treatment (MAT) has demonstrated 70% retention rates at 12 months, showing effectiveness for opioid use disorders when appropriate screening and monitoring protocols are in place.6
Stepwise outpatient detox may be suitable for select patients, particularly those who have strong social support and reliable engagement with medical care. However, providers must use careful clinical assessment to ensure safety, as outpatient settings cannot match the continuous monitoring available in inpatient care. The choice between outpatient treatment vs inpatient treatment for withdrawal management should be guided by the acuity of medical risk, history of withdrawal complications, and your capacity for safe community-based care.10
Recovery Starts With a Conversation
Whether you’re exploring recovery for yourself or seeking guidance for someone you care about, Coastal Recovery Partners is here to help. Our team offers trauma-informed, evidence-based support grounded in structure, compassion, and real connection—without pressure or judgment.
When you’re ready, we’ll meet you where you are and help you take the next step forward.
Professional and Lifestyle Considerations
Employment Continuity and Career Impact
Outpatient treatment excels at preserving your employment status and career trajectory.
Employment continuity is a critical differentiator when evaluating outpatient treatment vs inpatient treatment for working professionals. Outpatient programs are structured to support ongoing work engagement, offering therapy and medical management at times that do not disrupt professional obligations. Data from the Substance Abuse and Mental Health Services Administration indicate that 66% of individuals in outpatient programs maintain employment throughout treatment, compared to marked employment disruption during inpatient stays.7
The benefits of outpatient flexibility for professionals include:
- Sustaining regular income and financial stability.
- Meeting workplace responsibilities without raising red flags.
- Avoiding extended absences that could jeopardize career advancement or require complex HR disclosures.
- Applying coping skills learned in therapy directly to real-world workplace stressors.
Many professionals manage their treatment schedules digitally to seamlessly blend care with their work week. For instance, a typical outpatient schedule might look like this:
Example: Professional IOP Treatment Schedule
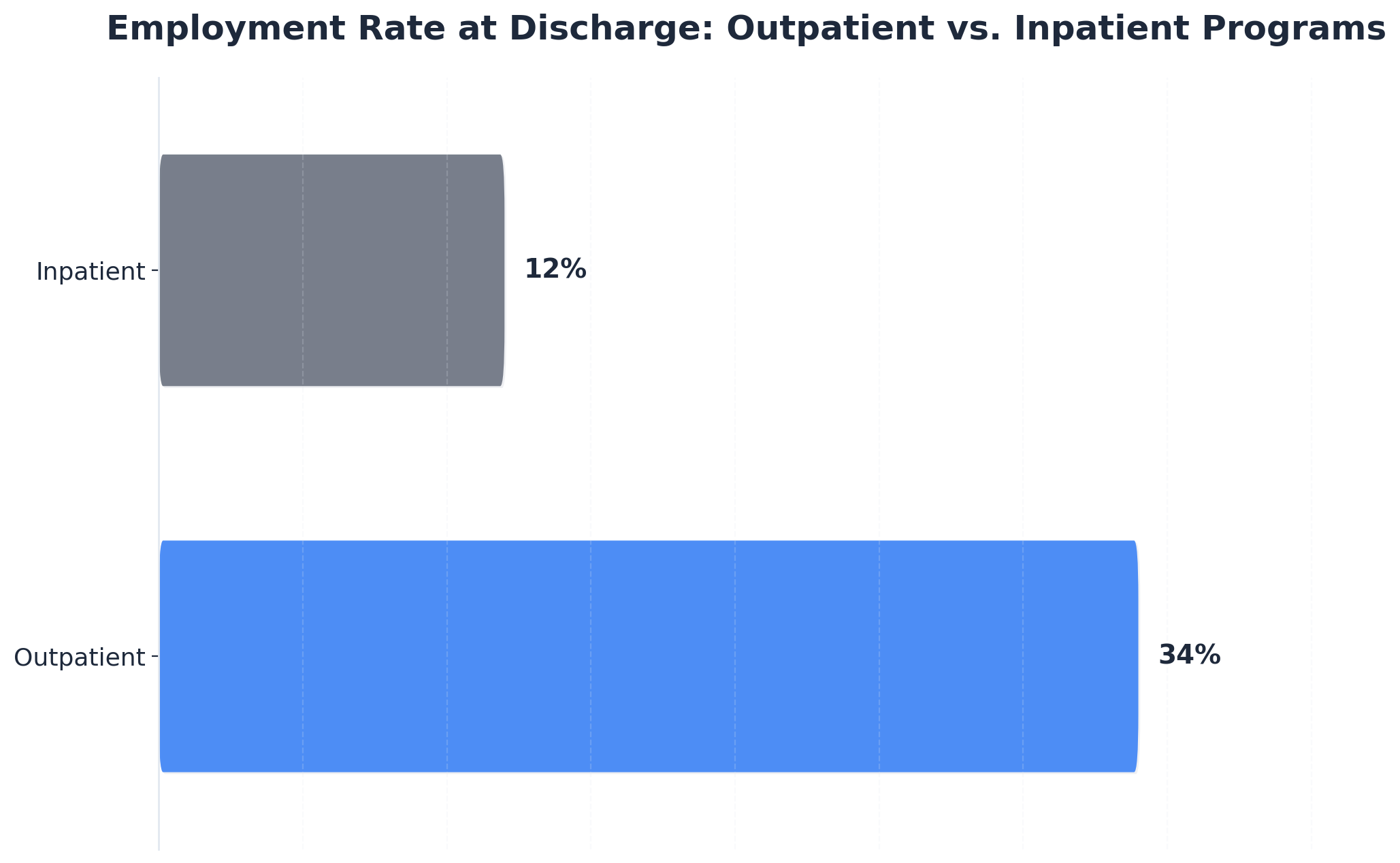
In contrast, inpatient treatment requires full-time residence, leading to a temporary withdrawal from the workforce. While this setting provides intensive clinical oversight, it often necessitates formal medical leave or short-term disability filings, and can create gaps in workplace continuity. National outcome measures show that only 12% of those exiting inpatient care report being employed at discharge, reflecting the significant impact on occupational status during and immediately after residential treatment.3
Family Responsibilities and Social Support
Outpatient care excels when you have a strong, supportive home environment and active family roles.
Family responsibilities and social support play a pivotal role in determining whether outpatient treatment or inpatient treatment is the optimal fit for professionals managing addiction recovery. Outpatient models excel for those with strong family involvement and stable home environments, as you can remain present for caregiving, parenting, or other essential household roles while engaging in structured therapy. Data from a national helpline survey indicates that 71% of treatment seekers with dependents specifically prefer outpatient care, citing the need to maintain daily family routines as a deciding factor.5
Modern outpatient care also utilizes technology to make balancing these responsibilities easier. When logging into your patient portal from home, you might simply use Ctrl + D to bookmark your telehealth link, allowing you to transition from family dinner to a therapy session in minutes.
In contrast, inpatient treatment may be necessary when a home environment is unstable, unsafe, or lacks reliable social support. The immersive nature of residential care removes individuals from potentially triggering or unsupportive situations, providing a secure space for stabilization and intensive therapeutic work. This is especially relevant in cases where cohabiting family members are also struggling with substance use or when there is a heightened risk of relapse due to household dynamics.8
Research underscores that successful recovery is often linked to the quality of post-treatment social support; however, 60–80% of those entering inpatient programs report limited or problematic support networks, further justifying the need for temporary separation. When weighing outpatient treatment vs inpatient treatment, professionals should consider both the benefits of ongoing family engagement and the necessity of a safe, supportive recovery environment.8

Outpatient programs excel in long-term retention when care intensity matches your clinical needs and lifestyle.
Evidence-Based Outcomes and Effectiveness in Outpatient Treatment vs Inpatient Treatment
Treatment Completion and Retention Rates
When it comes to treatment completion and retention rates, outpatient treatment often demonstrates a clear advantage for individuals with stable living environments and reliable support systems. Data show that outpatient Medication-Assisted Treatment (MAT) programs achieve 70% retention at 12 months, which is comparable to or even higher than many inpatient settings, especially when outpatient intensity is matched to clinical need. Outpatient programs also benefit from flexible scheduling, enabling professionals to remain engaged with work and family, factors closely tied to higher program completion rates.6
In contrast, inpatient treatment excels for those facing acute psychiatric needs or unstable environments, as the immersive nature of residential care can support initial stabilization. However, completion rates in inpatient settings are strongly influenced by the severity of clinical presentation and external obligations; abrupt transitions back to daily life can lead to lower long-term retention unless there is coordinated follow-up care.9
These trends highlight the importance of matching treatment type to individual needs in the outpatient treatment vs inpatient treatment decision. The following section will examine how each modality impacts long-term recovery and quality of life.
Long-Term Recovery and Quality of Life
Outpatient care excels at facilitating seamless reintegration into your daily professional and personal life.
When evaluating long-term recovery and quality of life, outpatient treatment stands out for professionals who require ongoing work and family engagement. Research indicates that outpatient programs, especially those incorporating MAT, offer not only high retention but also superior reintegration outcomes.
"Patients in outpatient programs report a 34% employment rate at discharge, compared to just 12% for inpatient counterparts, demonstrating a clear link between outpatient care and occupational stability."3
This employment continuity is closely linked to long-term housing stability and reduced relapse risk. Inpatient treatment, by contrast, excels at stabilizing severe cases and managing acute psychiatric or medical crises. However, while short-term abstinence rates may be higher immediately post-discharge, studies reveal no significant difference in long-term sobriety between well-matched outpatient and inpatient populations when placement is guided by clinical need. The immersive structure of inpatient care can disrupt daily routines, sometimes creating challenges in rebuilding social and occupational roles after leaving the program.9
A key takeaway from the outpatient treatment vs inpatient treatment comparison is the importance of matching treatment intensity to each individual's circumstances and support systems. For professionals, the flexibility of outpatient care can enhance quality of life by preserving autonomy and social connections, while inpatient care remains vital for those needing comprehensive stabilization.
Conclusion
For professionals navigating recovery while maintaining career responsibilities, the path forward requires both clinical excellence and practical accessibility. The treatment field has evolved to recognize that recovery outcomes improve significantly when programs align with the realities of professional life rather than requiring individuals to step away from their careers entirely.
Choose outpatient treatment if you have a stable home environment, manageable withdrawal symptoms, and need to maintain your career and family obligations. Structured outpatient programming addresses this need through flexible scheduling frameworks—morning, afternoon, and evening sessions that integrate with work commitments rather than displacing them. The clinical components remain comprehensive: evidence-based modalities including CBT, DBT, and motivational interviewing form the therapeutic foundation, while medication-assisted treatment protocols provide pharmacological support when clinically indicated. Integrated dual diagnosis care ensures co-occurring conditions receive concurrent attention within a unified, trauma-informed treatment plan, eliminating the fragmentation that often undermines outcomes.
Choose inpatient treatment if you require 24/7 medical supervision for acute withdrawal, lack a safe living situation, or are experiencing a severe psychiatric crisis that demands immediate, immersive stabilization.
The field continues to demonstrate that accessibility directly correlates with engagement and long-term success. Programs designed around professional schedules acknowledge that sustainable recovery depends on removing structural barriers to treatment participation. Coastal Recovery Partners provides this framework through Intensive Outpatient, Partial Hospitalization, and standard Outpatient programs in South Portland, Maine. With dedicated care coordination services and insurance navigation support, we streamline access for professionals seeking evidence-based treatment without career interruption.
Remember that recovery is a journey of rebuilding trust—in yourself, in others, and in the process of healing. If you are ready to explore your options, reach out to Coastal Recovery today. We're here to help guide you toward a future defined not by your past, but by your resilience and hope.

Frequently Asked Questions
Can someone transition from inpatient to outpatient treatment mid-program?
Yes, transitioning from inpatient to outpatient treatment mid-program is clinically appropriate when a patient achieves stability and meets specific criteria for reduced supervision. This step-down approach, known as a continuum of care, is supported by research indicating that matching treatment intensity to current clinical needs improves outcomes—outpatient treatment completion rates increase by 23–31% when intensity is properly aligned. The decision is typically made by the treatment team using comprehensive biopsychosocial assessments to ensure safety, readiness, and adequate support. The transition allows ongoing therapy, relapse prevention, and medication management while enabling professionals to resume daily responsibilities in the outpatient setting.6
How do insurance requirements differ between outpatient and inpatient treatment authorization?
Insurance requirements for outpatient treatment vs inpatient treatment differ in both process and documentation. Inpatient treatment typically requires pre-authorization with detailed clinical justification, including evidence of severe substance use disorder, acute withdrawal risk, or unsafe home environments. Insurers often mandate daily or weekly medical necessity reviews for continued inpatient coverage. Outpatient treatment authorization is generally less restrictive, with many plans approving Intensive Outpatient (IOP) or Partial Hospitalization (PHP) based on standardized assessment tools and progress reports. Recent policy shifts increasingly favor evidence-based placement, requiring documentation that outpatient care is not only appropriate but also matches clinical need, rather than defaulting to inpatient first.3,4
What happens if outpatient treatment proves insufficient after starting?
If outpatient treatment proves insufficient after starting, a reassessment is conducted to determine the need for increased support or a higher level of care. This might involve transitioning to an Intensive Outpatient Program (IOP), Partial Hospitalization Program (PHP), or, when clinically indicated, moving to inpatient treatment for greater structure and safety. Research emphasizes that matching treatment intensity to patient needs is essential—outpatient completion rates improve by 23–31% when the level of care is adjusted to fit clinical severity. Communication among the treatment team and ongoing monitoring help ensure timely changes, prioritizing safety and optimal recovery outcomes for professionals.6
Can medication-assisted treatment be initiated in an outpatient setting without prior inpatient detox?
Yes, medication-assisted treatment (MAT) can be initiated in an outpatient setting without prior inpatient detoxification, provided the individual is medically stable and withdrawal symptoms are expected to be mild to moderate. Clinical protocols recommend a thorough assessment to determine suitability for outpatient MAT, especially for opioid use disorder. Studies show that outpatient MAT programs achieve a 70% retention rate at 12 months, comparable to or better than inpatient outcomes when appropriate monitoring and support are present. However, for those with severe withdrawal risk or unstable medical conditions, inpatient detox may still be necessary before transitioning to outpatient care.6
How do treatment schedules accommodate shift workers or non-traditional work hours?
Outpatient programs are specifically designed to accommodate professionals with shift work or non-traditional schedules by offering therapy and medical appointments at a range of times—including mornings, afternoons, evenings, and weekends. This flexibility is a key reason why 71% of individuals seeking addiction care, particularly those with work and family obligations, express a preference for outpatient treatment vs inpatient treatment. Inpatient programs, by contrast, follow a fixed daily schedule within the facility, making it difficult to maintain outside work responsibilities. For shift workers, outpatient models allow continued employment and consistent engagement in care, supporting both clinical outcomes and occupational stability.5
What role does telehealth play in outpatient versus inpatient treatment models?
Telehealth has become a major asset in outpatient treatment, enabling professionals to access therapy, medication management, and relapse prevention support from home or work. In outpatient settings, telehealth platforms increase flexibility and reduce logistical barriers, making it easier for working professionals to attend sessions without interrupting their schedules. Studies from 2024 highlight that telehealth integration in outpatient addiction care has preserved treatment engagement and retention, especially for those balancing work and family. In contrast, telehealth generally plays a minimal role in inpatient treatment, as care is delivered on-site with direct supervision. The outpatient treatment vs inpatient treatment distinction is clear: telehealth is a core feature in outpatient models, supporting continuity and accessibility.6
References
- 2021 National Survey on Drug Use and Health: State Estimates of Substance Use and Mental Illness - SAMHSA. https://www.samhsa.gov/data/sites/default/files/reports/rpt29393/2021-nsduh-sae-highlights.pdf
- Principles of Drug Addiction Treatment: A Research-Based Guide - National Institute on Drug Abuse. https://www.nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/principles-effective-treatment
- National Outcomes Measures (NOMs) for Substance Use and Mental Health Services - SAMHSA. https://www.samhsa.gov/sites/default/files/programs_campaigns/nsmhwb_data_outcomes_2017.pdf
- Barriers to Behavioral Health Treatment and Services - U.S. Department of Health and Human Services. https://aspe.hhs.gov/sites/default/files/private/pdf/264406/ous_bpd_white_paper_finalversion.pdf
- National Helpline Survey Data - SAMHSA. https://www.samhsa.gov/data/sites/default/files/reports/rpt8969/2020-samhsa-national-helpline-survey.pdf
- How is Opioid Addiction Treated? - National Institute on Drug Abuse. https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-is-opioid-addiction-treated
- CDC Drug Overdose Surveillance Report 2021 - Centers for Disease Control and Prevention. https://www.cdc.gov/drugoverdose/pdf/pubs/2021-odr-surveillance-report.pdf
- Guide to Evidence-Based Comprehensive Addiction Treatment - SAMHSA. https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP19-02-00-001.pdf
- Comparative Effectiveness of Addiction Treatment Modalities in Outpatient and Inpatient Settings - PubMed Central. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6526724/
- Medication-Assisted Treatment for Substance Use Disorders: Clinical and Health Policy Outcomes - HHS ASPE. https://aspe.hhs.gov/sites/default/files/private/pdf/263666/medication-assisted-treatment-report-2.pdf
- Google Scholar. https://scholar.google.com
- PubMed. https://pubmed.ncbi.nlm.nih.gov



